Rebecca C. Rossom MD , A. Lauren Crain PhD , Gavin Bart MD , Julie E. Richards PhD , Jennifer M. Boggs PhD , Patrick J. O'Connor MD , Caitlin Borgert-Spaniol MA , Sheryl Kane MS , Stephanie A. Hooker PhD
{"title":"随机试用临床决策支持工具,加强对有阿片类药物使用障碍的高危初级保健患者的自杀筛查","authors":"Rebecca C. Rossom MD , A. Lauren Crain PhD , Gavin Bart MD , Julie E. Richards PhD , Jennifer M. Boggs PhD , Patrick J. O'Connor MD , Caitlin Borgert-Spaniol MA , Sheryl Kane MS , Stephanie A. Hooker PhD","doi":"10.1016/j.focus.2024.100280","DOIUrl":null,"url":null,"abstract":"<div><h3>Introduction</h3><div>Individuals with opioid use disorder are at elevated suicide risk, but systematic screening in this population is rarely done. This study assessed the effects of targeted clinical decision support prompts on structured suicide risk assessment completion.</div></div><div><h3>Methods</h3><div>The study used a cluster-randomized controlled pragmatic pilot design. Adult primary care patients (aged 18–75 years) with or at risk for opioid use disorder or opioid overdose and suicide were eligible. Patients sought care from 15 Midwestern primary care clinics between July, 31, 2021 and July, 31, 2022. Data were analyzed between March and June 2023. Clinicians in intervention and control clinics received a printout from rooming staff, prompted by a clinical decision support-generated electronic health record alert, suggesting clinicians talk with patients about opioid risks. Intervention clinician handouts also alerted them to patients estimated to be at increased suicide risk and recommended completion of a Columbia Suicide Severity Rating Scale to further evaluate suicide risk. The handouts for control clinicians did not include suicide risk alerts. The main outcome measured the completion of the Columbia Suicide Severity Rating Scale in the 14 days following a visit.</div></div><div><h3>Results</h3><div>A total of 115 eligible patients (69 intervention, 46 control) made at least 1 visit to a randomized clinic. Patients mean age was 39 years, and 57% were women; 48% of patients had a high risk of opioid use disorder or opioid overdose, 39% had an opioid use disorder diagnosis, 12% had an opioid use disorder in remission diagnosis, and 5% had a recent opioid overdose. Over a mean follow-up of 249 days, 20.3% of intervention patients and 17.4% of control patients had at least 1 Columbia Suicide Severity Rating Scale completed in the next 14 days (<em>p</em>=0.70). Most (71%–75%) Columbia Suicide Severity Rating Scale scores were 0, indicating no risk.</div></div><div><h3>Conclusions</h3><div>This pilot study did not increase the uptake of structured suicide risk assessments in primary care for patients at elevated risk for opioid use disorder and suicide. More robust interventions are likely needed to promote suicide risk assessment in primary care.</div></div>","PeriodicalId":72142,"journal":{"name":"AJPM focus","volume":"3 6","pages":"Article 100280"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Randomized Pilot of a Clinical Decision Support Tool to Increase Suicide Screening for at-Risk Primary Care Patients With Opioid Use Disorder\",\"authors\":\"Rebecca C. Rossom MD , A. Lauren Crain PhD , Gavin Bart MD , Julie E. Richards PhD , Jennifer M. Boggs PhD , Patrick J. O'Connor MD , Caitlin Borgert-Spaniol MA , Sheryl Kane MS , Stephanie A. Hooker PhD\",\"doi\":\"10.1016/j.focus.2024.100280\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Introduction</h3><div>Individuals with opioid use disorder are at elevated suicide risk, but systematic screening in this population is rarely done. This study assessed the effects of targeted clinical decision support prompts on structured suicide risk assessment completion.</div></div><div><h3>Methods</h3><div>The study used a cluster-randomized controlled pragmatic pilot design. Adult primary care patients (aged 18–75 years) with or at risk for opioid use disorder or opioid overdose and suicide were eligible. Patients sought care from 15 Midwestern primary care clinics between July, 31, 2021 and July, 31, 2022. Data were analyzed between March and June 2023. Clinicians in intervention and control clinics received a printout from rooming staff, prompted by a clinical decision support-generated electronic health record alert, suggesting clinicians talk with patients about opioid risks. Intervention clinician handouts also alerted them to patients estimated to be at increased suicide risk and recommended completion of a Columbia Suicide Severity Rating Scale to further evaluate suicide risk. The handouts for control clinicians did not include suicide risk alerts. The main outcome measured the completion of the Columbia Suicide Severity Rating Scale in the 14 days following a visit.</div></div><div><h3>Results</h3><div>A total of 115 eligible patients (69 intervention, 46 control) made at least 1 visit to a randomized clinic. Patients mean age was 39 years, and 57% were women; 48% of patients had a high risk of opioid use disorder or opioid overdose, 39% had an opioid use disorder diagnosis, 12% had an opioid use disorder in remission diagnosis, and 5% had a recent opioid overdose. Over a mean follow-up of 249 days, 20.3% of intervention patients and 17.4% of control patients had at least 1 Columbia Suicide Severity Rating Scale completed in the next 14 days (<em>p</em>=0.70). Most (71%–75%) Columbia Suicide Severity Rating Scale scores were 0, indicating no risk.</div></div><div><h3>Conclusions</h3><div>This pilot study did not increase the uptake of structured suicide risk assessments in primary care for patients at elevated risk for opioid use disorder and suicide. More robust interventions are likely needed to promote suicide risk assessment in primary care.</div></div>\",\"PeriodicalId\":72142,\"journal\":{\"name\":\"AJPM focus\",\"volume\":\"3 6\",\"pages\":\"Article 100280\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-10-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"AJPM focus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://www.sciencedirect.com/science/article/pii/S2773065424000981\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"AJPM focus","FirstCategoryId":"1085","ListUrlMain":"https://www.sciencedirect.com/science/article/pii/S2773065424000981","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
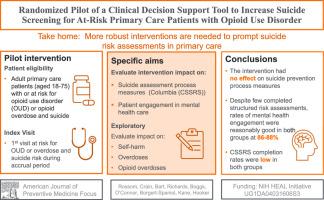
Randomized Pilot of a Clinical Decision Support Tool to Increase Suicide Screening for at-Risk Primary Care Patients With Opioid Use Disorder
Introduction
Individuals with opioid use disorder are at elevated suicide risk, but systematic screening in this population is rarely done. This study assessed the effects of targeted clinical decision support prompts on structured suicide risk assessment completion.
Methods
The study used a cluster-randomized controlled pragmatic pilot design. Adult primary care patients (aged 18–75 years) with or at risk for opioid use disorder or opioid overdose and suicide were eligible. Patients sought care from 15 Midwestern primary care clinics between July, 31, 2021 and July, 31, 2022. Data were analyzed between March and June 2023. Clinicians in intervention and control clinics received a printout from rooming staff, prompted by a clinical decision support-generated electronic health record alert, suggesting clinicians talk with patients about opioid risks. Intervention clinician handouts also alerted them to patients estimated to be at increased suicide risk and recommended completion of a Columbia Suicide Severity Rating Scale to further evaluate suicide risk. The handouts for control clinicians did not include suicide risk alerts. The main outcome measured the completion of the Columbia Suicide Severity Rating Scale in the 14 days following a visit.
Results
A total of 115 eligible patients (69 intervention, 46 control) made at least 1 visit to a randomized clinic. Patients mean age was 39 years, and 57% were women; 48% of patients had a high risk of opioid use disorder or opioid overdose, 39% had an opioid use disorder diagnosis, 12% had an opioid use disorder in remission diagnosis, and 5% had a recent opioid overdose. Over a mean follow-up of 249 days, 20.3% of intervention patients and 17.4% of control patients had at least 1 Columbia Suicide Severity Rating Scale completed in the next 14 days (p=0.70). Most (71%–75%) Columbia Suicide Severity Rating Scale scores were 0, indicating no risk.
Conclusions
This pilot study did not increase the uptake of structured suicide risk assessments in primary care for patients at elevated risk for opioid use disorder and suicide. More robust interventions are likely needed to promote suicide risk assessment in primary care.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


