在猪难治性心脏骤停实验模型中,除体外生命支持外,胸外按压对颈动脉血流的影响
IF 2.1
Q3 CRITICAL CARE MEDICINE
引用次数: 0
摘要
背景体外生命支持(ECLS)可为难治性心脏骤停患者提供器官灌注,但在启动 ECLS 期间,平均动脉压(MAP)和颈动脉血流可能会因低血压和/或血流不足而达不到最佳状态。我们假设,与单独使用 ECLS 相比,在使用 ECLS 的同时使用心肺复苏术(CPR)可能会增加颈动脉血流量和 MAP。对猪进行麻醉,诱导室颤 3 分钟,自动心肺复苏 30 分钟,启动 ECLS,然后停止心肺复苏。比较心肺复苏 + ECLS 最后 3 秒钟与单独 ECLS 的 3、6、30 秒钟以及 5 和 10 分钟之间 3 秒钟的平均变量。数据以中位数(25-75 四分位数间距)表示,并使用配对样本 Wilcoxon 检验进行比较。心肺复苏+ECLS时的血压为56(53.0-59.2)毫米汞柱,而单独使用ECLS时分别为50(45-57)毫米汞柱、52(46-59)毫米汞柱、61(50-63)毫米汞柱、57(54-66)毫米汞柱、54(47-58)毫米汞柱,P分别为0.50、0.61、0.70、0.44、0.73。心肺复苏+ECLS时的颈动脉血流量为113(78-119)毫升/分钟,而单用ECLS时分别为99(79-110)毫升/分钟、100(81-110)毫升/分钟、96(60-122)毫升/分钟、118(101-130)毫升/分钟、124(110-141)毫升/分钟,p分别为0.41、0.52、0.73、0.33、0.20。结论在有效启动 ECLS 后停止 CPR 不会降低 MAP 或颈动脉血流量。未来的研究可能会评估用心肺复苏增强低流量 ECLS 的效果。本文章由计算机程序翻译,如有差异,请以英文原文为准。
Effect of chest compressions in addition to extracorporeal life support on carotid flow in an experimental model of refractory cardiac arrest in pigs
Background
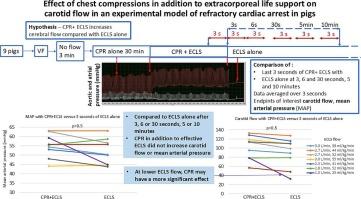
Extracorporeal life support (ECLS) provides organ perfusion in refractory cardiac arrest but during the initiation of ECLS mean arterial pressure (MAP) and carotid flow may be suboptimal due to hypotension and/or insufficient flow. We hypothesized that cardiopulmonary resuscitation (CPR) in addition to ECLS may increase carotid flow and MAP compared to ECLS alone.
Methods
Observational pilot study comparing hemodynamic parameters before and after CPR cessation in pigs supported by ECLS for experimental refractory cardiac arrest. Pigs were anesthetized, ventricular fibrillation was induced for 3 min, automated CPR performed for 30 min, ECLS was initiated then CPR stopped.
Variables averaged over 3 s were compared between the last 3 s of CPR + ECLS and 3, 6, 30 s, and 5 and 10 min of ECLS alone. Data are expressed as medians (25–75 interquartile range) and compared using paired samples Wilcoxon test.
Results
Nine pigs were included, ECLS was initiated at 2.7 (2.3–2.8) L/min. MAP during CPR + ECLS was 56(53.0–59.2) mmHg, versus 50(45–57)mmHg, 52(46–59)mmHg, 61(50–63)mmHg, 57 (54–66)mmHg, 54 (47–58)mmHg of ECLS alone, p = 0.50, 0.61, 0.70, 0.44, 0.73 respectively. Carotid flow was 113(78–119) ml/min during CPR + ECLS versus 99(79–110)ml/min, 100(81–110)ml/min, 96(60–122)ml/min, 118 (101–130)ml/min, 124 (110–141)ml/min, p = 0.41, 0.52, 0.73, 0.33, 0.20 respectively. When ECLS was initiated at lower flow, 1.5 L/min (one pig), MAP decreased from 59 to 45 mmHg, and carotid flow from 78.2 to 32.5 ml/min after 3 s of ECLS alone.
Conclusion
Stopping CPR after effective ECLS initiation does not decrease MAP or carotid flow. Future studies may evaluate augmenting low flow ECLS with CPR.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊

Resuscitation plus
Critical Care and Intensive Care Medicine, Emergency Medicine
CiteScore
3.00
自引率
0.00%
发文量
0
审稿时长
52 days
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


