{"title":"慢性肺水肿急性加重期的成功治疗:病例报告。","authors":"Junichi Morimoto, Taiki Fujiwara, Ryo Karita, Jotaro Yusa, Mitsutoshi Shiba, Tomohiko Iida","doi":"10.1186/s44215-024-00151-9","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Most cases of chronic empyema are caused by acute thoracic empyema or tuberculous pleuritis. Open thoracotomy and decortication are traditional treatments for chronic empyema. However, some cases, such as those with thick calcifications around a large cavity, may be difficult to decorticate in a single surgery. We successfully treated a case of chronic empyema with a large cavity surrounded by a thick calcified membrane that was peeled off gradually each day through fenestration of the thoracic cavity with negative-pressure wound therapy (NPWT).</p><p><strong>Case presentation: </strong>The patient was a 47-year-old man who had undergone thoracic drainage for left post-pneumonia empyema at another hospital 10 years previously. He presented to our hospital with a fever of 39 °C, bloody sputum, and severe fatigue for 3 days. Computed tomography showed a 9-cm mass shadow in the left intralobar space and an adjacent 21 × 15 × 9-cm fluid-filled calcified unilocular cavity up to 5 mm in thickness. He underwent thoracic drainage for fluid, and empyema was suspected; the fluid was foul-smelling and purulent. The patient did not improve with antibiotics and intrathoracic lavage; therefore, thoracoscopic decortication was performed. The thoracic cavity had a thick calcified membrane filled with dark-red slurry resembling old blood. We attempted decortication; however, the calcified membrane was difficult to remove. Two drains were used for the pleural lavage. However, no improvement was observed with intrathoracic lavage and drainage; therefore, a fenestration was performed. The calcified membrane was peeled off each day for 3 months. Gradually, granulation increased and the inflammatory reaction improved. After NPWT, the empyema cavity gradually shrank to 8 cm × 6 cm × 2 cm. A latissimus dorsi flap closure was performed, and the patient was discharged.</p><p><strong>Conclusions: </strong>This is an informative report on the daily decortication of a highly calcified purulent membrane using NPWT in a patient with chronic empyema. The description of this method will aid in the management of patients with chronic empyema and thick calcified membranes.</p>","PeriodicalId":520286,"journal":{"name":"General Thoracic and Cardiovascular Surgery Cases","volume":"3 1","pages":"30"},"PeriodicalIF":0.1000,"publicationDate":"2024-05-27","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533538/pdf/","citationCount":"0","resultStr":"{\"title\":\"Successful treatment with fenestration followed by daily decortication and negative-pressure wound therapy for acute exacerbation of chronic empyema: a case report.\",\"authors\":\"Junichi Morimoto, Taiki Fujiwara, Ryo Karita, Jotaro Yusa, Mitsutoshi Shiba, Tomohiko Iida\",\"doi\":\"10.1186/s44215-024-00151-9\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Most cases of chronic empyema are caused by acute thoracic empyema or tuberculous pleuritis. Open thoracotomy and decortication are traditional treatments for chronic empyema. However, some cases, such as those with thick calcifications around a large cavity, may be difficult to decorticate in a single surgery. We successfully treated a case of chronic empyema with a large cavity surrounded by a thick calcified membrane that was peeled off gradually each day through fenestration of the thoracic cavity with negative-pressure wound therapy (NPWT).</p><p><strong>Case presentation: </strong>The patient was a 47-year-old man who had undergone thoracic drainage for left post-pneumonia empyema at another hospital 10 years previously. He presented to our hospital with a fever of 39 °C, bloody sputum, and severe fatigue for 3 days. Computed tomography showed a 9-cm mass shadow in the left intralobar space and an adjacent 21 × 15 × 9-cm fluid-filled calcified unilocular cavity up to 5 mm in thickness. He underwent thoracic drainage for fluid, and empyema was suspected; the fluid was foul-smelling and purulent. The patient did not improve with antibiotics and intrathoracic lavage; therefore, thoracoscopic decortication was performed. The thoracic cavity had a thick calcified membrane filled with dark-red slurry resembling old blood. We attempted decortication; however, the calcified membrane was difficult to remove. Two drains were used for the pleural lavage. However, no improvement was observed with intrathoracic lavage and drainage; therefore, a fenestration was performed. The calcified membrane was peeled off each day for 3 months. Gradually, granulation increased and the inflammatory reaction improved. After NPWT, the empyema cavity gradually shrank to 8 cm × 6 cm × 2 cm. A latissimus dorsi flap closure was performed, and the patient was discharged.</p><p><strong>Conclusions: </strong>This is an informative report on the daily decortication of a highly calcified purulent membrane using NPWT in a patient with chronic empyema. The description of this method will aid in the management of patients with chronic empyema and thick calcified membranes.</p>\",\"PeriodicalId\":520286,\"journal\":{\"name\":\"General Thoracic and Cardiovascular Surgery Cases\",\"volume\":\"3 1\",\"pages\":\"30\"},\"PeriodicalIF\":0.1000,\"publicationDate\":\"2024-05-27\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533538/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"General Thoracic and Cardiovascular Surgery Cases\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s44215-024-00151-9\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"General Thoracic and Cardiovascular Surgery Cases","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s44215-024-00151-9","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"","JCRName":"","Score":null,"Total":0}
Successful treatment with fenestration followed by daily decortication and negative-pressure wound therapy for acute exacerbation of chronic empyema: a case report.
Background: Most cases of chronic empyema are caused by acute thoracic empyema or tuberculous pleuritis. Open thoracotomy and decortication are traditional treatments for chronic empyema. However, some cases, such as those with thick calcifications around a large cavity, may be difficult to decorticate in a single surgery. We successfully treated a case of chronic empyema with a large cavity surrounded by a thick calcified membrane that was peeled off gradually each day through fenestration of the thoracic cavity with negative-pressure wound therapy (NPWT).
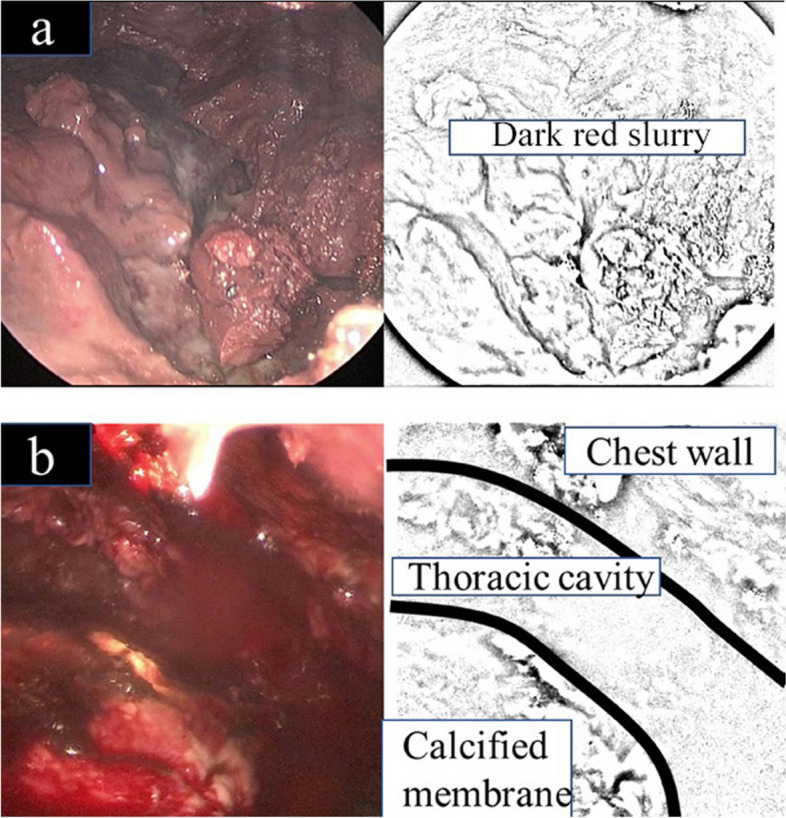
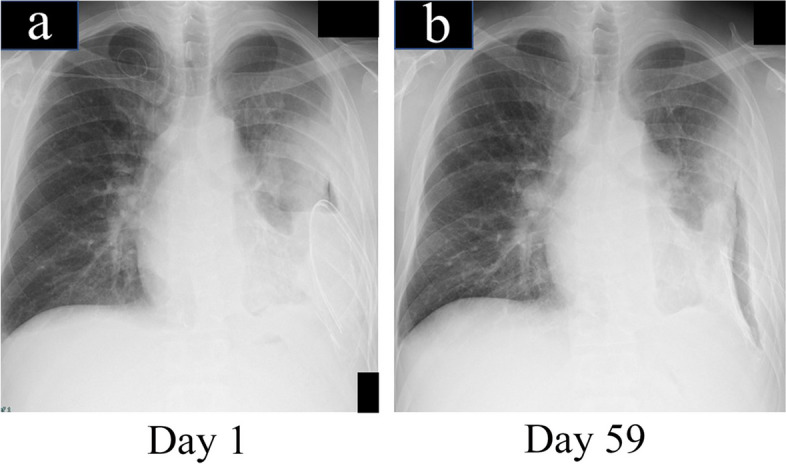
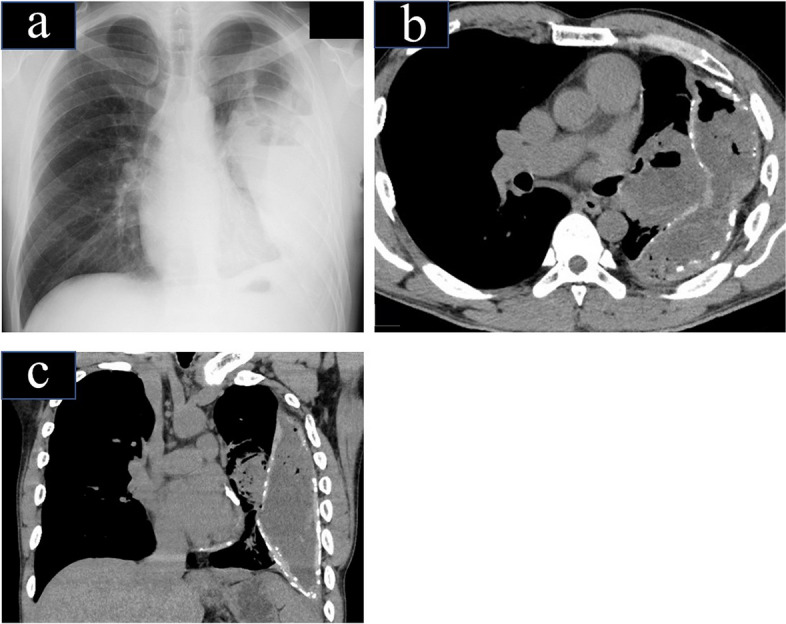
Case presentation: The patient was a 47-year-old man who had undergone thoracic drainage for left post-pneumonia empyema at another hospital 10 years previously. He presented to our hospital with a fever of 39 °C, bloody sputum, and severe fatigue for 3 days. Computed tomography showed a 9-cm mass shadow in the left intralobar space and an adjacent 21 × 15 × 9-cm fluid-filled calcified unilocular cavity up to 5 mm in thickness. He underwent thoracic drainage for fluid, and empyema was suspected; the fluid was foul-smelling and purulent. The patient did not improve with antibiotics and intrathoracic lavage; therefore, thoracoscopic decortication was performed. The thoracic cavity had a thick calcified membrane filled with dark-red slurry resembling old blood. We attempted decortication; however, the calcified membrane was difficult to remove. Two drains were used for the pleural lavage. However, no improvement was observed with intrathoracic lavage and drainage; therefore, a fenestration was performed. The calcified membrane was peeled off each day for 3 months. Gradually, granulation increased and the inflammatory reaction improved. After NPWT, the empyema cavity gradually shrank to 8 cm × 6 cm × 2 cm. A latissimus dorsi flap closure was performed, and the patient was discharged.
Conclusions: This is an informative report on the daily decortication of a highly calcified purulent membrane using NPWT in a patient with chronic empyema. The description of this method will aid in the management of patients with chronic empyema and thick calcified membranes.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


