Thomas Cho, Amy Waters, Shiva Senthilkumar, Shradha Shendge, Jiayong Liu
{"title":"动态固定与静态固定和腓骨钉治疗联合踝关节骨折的疗效比较:一项荟萃分析和系统综述。","authors":"Thomas Cho, Amy Waters, Shiva Senthilkumar, Shradha Shendge, Jiayong Liu","doi":"10.21037/aoj-24-14","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Syndesmotic ankle fractures occur when there is damage to the syndesmosis complex, resulting in severe pain and instability. Treatment methods include static fixation, dynamic fixation, and fibular nailing. This systematic review and meta-analysis aims to compare the outcomes of these surgical interventions for syndesmotic ankle fractures.</p><p><strong>Methods: </strong>PubMed and Embase were searched up until April 2024 for comparison studies that included at least two of the treatment methods and relevant functional outcomes and complication metrics. Review Manager 5.4 was used for statistical analyses, and a P value ≤0.05 was considered statistically significant. Risk of bias was assessed with Review Manager 5.4. and the Newcastle-Ottawa scale.</p><p><strong>Results: </strong>Nineteen studies with a total of 1,182 patients met the inclusion criteria. Compared to static fixation, dynamic fixation had a significantly higher Olerud-Molander Ankle Score (OMAS) at both 1-year [standardized mean difference (SMD) =0.43; 95% confidence interval (CI): 0.22 to 0.65; P<0.05] and 2-year post-operation (SMD =0.76; 95% CI: 0.33 to 1.20; P<0.05). Dynamic fixation had a significantly lower reoperation rate than static fixation [risk ratio (RR) =0.55; 95% CI: 0.36 to 0.83; P=0.004]. Compared to static fixation, fibular nail had a significantly higher OMAS at 1-year post-operation (SMD =0.28; 95% CI: 0.03 to 0.53; P=0.03). Fibular nails had significantly lower infection (RR =0.12; 95% CI: 0.04 to 0.37; P<0.05) and reoperation rates (RR =0.22; 95% CI: 0.06 to 0.86; P=0.03) than static fixation. Compared to fibular nail, dynamic fixation had a significantly higher OMAS at both 1-year (SMD =1.07; 95% CI: 0.83 to 1.31; P<0.05) and 2-year post-operation (SMD =1.03; 95% CI: 0.60 to 1.47; P<0.05). Dynamic fixation had a significantly higher reoperation rate compared to fibular nail (RR =20.41; 95% CI: 2.81 to 148.21; P=0.003).</p><p><strong>Conclusions: </strong>Dynamic fixation seems to be the superior treatment method, displaying better outcomes than static fixation and fibular nailing, with the fibular nail proving to be a viable alternative. Dynamic fixation should be the first choice of treatment for those with syndesmotic ankle fractures due to its clinical advantages compared to static fixation and fibular nailing.</p><p><strong>Level of evidence: </strong>3.</p>","PeriodicalId":44459,"journal":{"name":"Annals of Joint","volume":"9 ","pages":"36"},"PeriodicalIF":0.9000,"publicationDate":"2024-09-06","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558278/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of the outcomes of syndesmotic ankle fractures treated with dynamic fixation versus static fixation versus fibular nail: a meta-analysis and systematic review.\",\"authors\":\"Thomas Cho, Amy Waters, Shiva Senthilkumar, Shradha Shendge, Jiayong Liu\",\"doi\":\"10.21037/aoj-24-14\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Syndesmotic ankle fractures occur when there is damage to the syndesmosis complex, resulting in severe pain and instability. Treatment methods include static fixation, dynamic fixation, and fibular nailing. This systematic review and meta-analysis aims to compare the outcomes of these surgical interventions for syndesmotic ankle fractures.</p><p><strong>Methods: </strong>PubMed and Embase were searched up until April 2024 for comparison studies that included at least two of the treatment methods and relevant functional outcomes and complication metrics. Review Manager 5.4 was used for statistical analyses, and a P value ≤0.05 was considered statistically significant. Risk of bias was assessed with Review Manager 5.4. and the Newcastle-Ottawa scale.</p><p><strong>Results: </strong>Nineteen studies with a total of 1,182 patients met the inclusion criteria. Compared to static fixation, dynamic fixation had a significantly higher Olerud-Molander Ankle Score (OMAS) at both 1-year [standardized mean difference (SMD) =0.43; 95% confidence interval (CI): 0.22 to 0.65; P<0.05] and 2-year post-operation (SMD =0.76; 95% CI: 0.33 to 1.20; P<0.05). Dynamic fixation had a significantly lower reoperation rate than static fixation [risk ratio (RR) =0.55; 95% CI: 0.36 to 0.83; P=0.004]. Compared to static fixation, fibular nail had a significantly higher OMAS at 1-year post-operation (SMD =0.28; 95% CI: 0.03 to 0.53; P=0.03). Fibular nails had significantly lower infection (RR =0.12; 95% CI: 0.04 to 0.37; P<0.05) and reoperation rates (RR =0.22; 95% CI: 0.06 to 0.86; P=0.03) than static fixation. Compared to fibular nail, dynamic fixation had a significantly higher OMAS at both 1-year (SMD =1.07; 95% CI: 0.83 to 1.31; P<0.05) and 2-year post-operation (SMD =1.03; 95% CI: 0.60 to 1.47; P<0.05). Dynamic fixation had a significantly higher reoperation rate compared to fibular nail (RR =20.41; 95% CI: 2.81 to 148.21; P=0.003).</p><p><strong>Conclusions: </strong>Dynamic fixation seems to be the superior treatment method, displaying better outcomes than static fixation and fibular nailing, with the fibular nail proving to be a viable alternative. Dynamic fixation should be the first choice of treatment for those with syndesmotic ankle fractures due to its clinical advantages compared to static fixation and fibular nailing.</p><p><strong>Level of evidence: </strong>3.</p>\",\"PeriodicalId\":44459,\"journal\":{\"name\":\"Annals of Joint\",\"volume\":\"9 \",\"pages\":\"36\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-09-06\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11558278/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Joint\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.21037/aoj-24-14\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Joint","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.21037/aoj-24-14","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Comparison of the outcomes of syndesmotic ankle fractures treated with dynamic fixation versus static fixation versus fibular nail: a meta-analysis and systematic review.
Background: Syndesmotic ankle fractures occur when there is damage to the syndesmosis complex, resulting in severe pain and instability. Treatment methods include static fixation, dynamic fixation, and fibular nailing. This systematic review and meta-analysis aims to compare the outcomes of these surgical interventions for syndesmotic ankle fractures.
Methods: PubMed and Embase were searched up until April 2024 for comparison studies that included at least two of the treatment methods and relevant functional outcomes and complication metrics. Review Manager 5.4 was used for statistical analyses, and a P value ≤0.05 was considered statistically significant. Risk of bias was assessed with Review Manager 5.4. and the Newcastle-Ottawa scale.
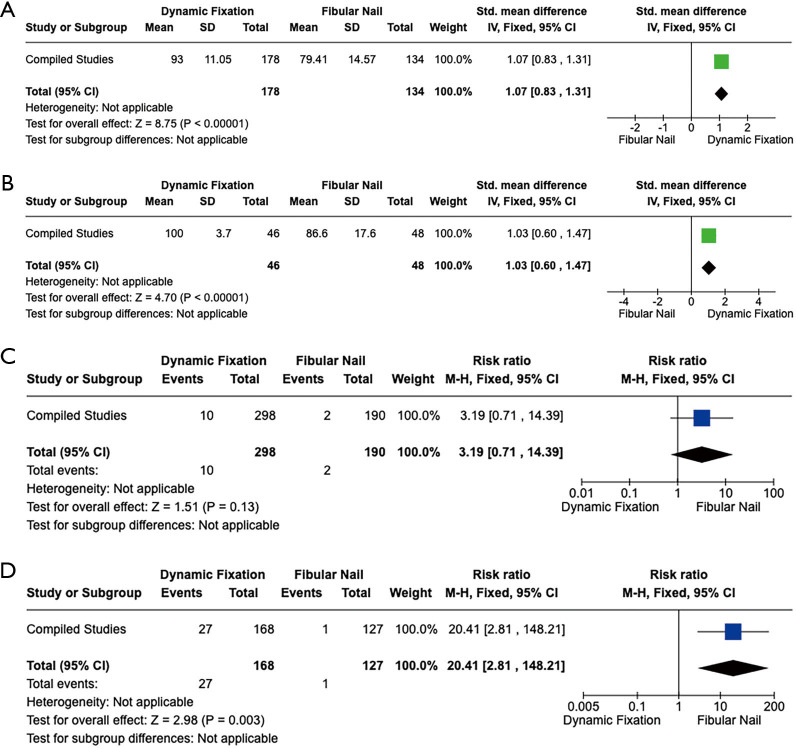
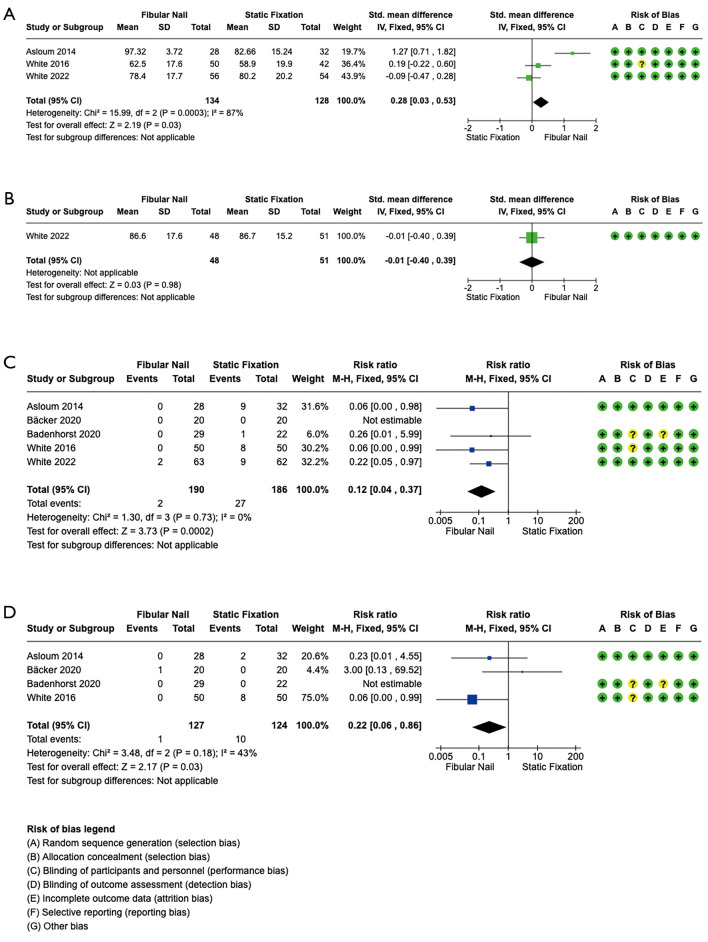
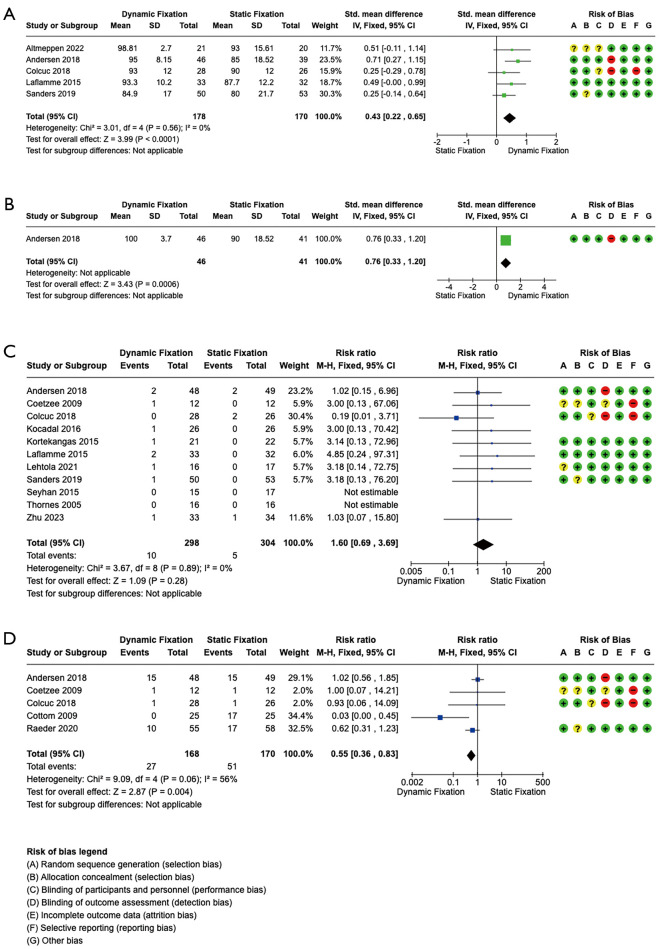
Results: Nineteen studies with a total of 1,182 patients met the inclusion criteria. Compared to static fixation, dynamic fixation had a significantly higher Olerud-Molander Ankle Score (OMAS) at both 1-year [standardized mean difference (SMD) =0.43; 95% confidence interval (CI): 0.22 to 0.65; P<0.05] and 2-year post-operation (SMD =0.76; 95% CI: 0.33 to 1.20; P<0.05). Dynamic fixation had a significantly lower reoperation rate than static fixation [risk ratio (RR) =0.55; 95% CI: 0.36 to 0.83; P=0.004]. Compared to static fixation, fibular nail had a significantly higher OMAS at 1-year post-operation (SMD =0.28; 95% CI: 0.03 to 0.53; P=0.03). Fibular nails had significantly lower infection (RR =0.12; 95% CI: 0.04 to 0.37; P<0.05) and reoperation rates (RR =0.22; 95% CI: 0.06 to 0.86; P=0.03) than static fixation. Compared to fibular nail, dynamic fixation had a significantly higher OMAS at both 1-year (SMD =1.07; 95% CI: 0.83 to 1.31; P<0.05) and 2-year post-operation (SMD =1.03; 95% CI: 0.60 to 1.47; P<0.05). Dynamic fixation had a significantly higher reoperation rate compared to fibular nail (RR =20.41; 95% CI: 2.81 to 148.21; P=0.003).
Conclusions: Dynamic fixation seems to be the superior treatment method, displaying better outcomes than static fixation and fibular nailing, with the fibular nail proving to be a viable alternative. Dynamic fixation should be the first choice of treatment for those with syndesmotic ankle fractures due to its clinical advantages compared to static fixation and fibular nailing.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


