{"title":"骨间后神经在不同肘部和前臂位置的体内动态迁移。","authors":"Kensuke Ikuta, Hideaki Miyamoto, Takahiro Inui, Hirotaka Kawano","doi":"10.5397/cise.2024.00213","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The posterior interosseous nerve (PIN) is at risk of iatrogenic nerve injury during elbow surgery when using a lateral or posterolateral approach. Results of cadaveric studies indicated that maintaining forearm pronation throughout the surgery can help move the PIN away from the surgical window. However, in vivo dynamic migration of the PIN in response to changes in the elbow and forearm position is unclear. This study aimed to clarify the in vivo dynamic migration pattern of the PIN in response to changes in the elbow and forearm position using ultrasound imaging.</p><p><strong>Methods: </strong>This study included 43 upper extremities of 22 healthy volunteers (16 females; mean age, 29 years). Using ultrasound imaging, we measured the shortest distance from the radial head (RH) to the point where the PIN crossed the lateral aspect of the radial axis in six positions of the elbow and forearm: 90° forearm supination, 90° pronation, and neutral forearm position, each at 135° of elbow flexion and 0° of elbow extension.</p><p><strong>Results: </strong>The RH-to-nerve distance was greater during elbow extension than during elbow flexion regardless of the forearm position. However, the maximum migration distance was 3.5 mm when transitioning from elbow extension and forearm pronation (25.1 mm) to elbow flexion and forearm supination (21.6 mm).</p><p><strong>Conclusions: </strong>Although forearm pronation may help move the PIN away from the surgical window, care should be taken not to injure the nerve when performing elbow surgery using a lateral or posterolateral approach. Level of evidence: III.</p>","PeriodicalId":33981,"journal":{"name":"Clinics in Shoulder and Elbow","volume":" ","pages":"407-411"},"PeriodicalIF":1.7000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11615462/pdf/","citationCount":"0","resultStr":"{\"title\":\"In vivo dynamic migration of the posterior interosseous nerve across various elbow and forearm positions.\",\"authors\":\"Kensuke Ikuta, Hideaki Miyamoto, Takahiro Inui, Hirotaka Kawano\",\"doi\":\"10.5397/cise.2024.00213\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The posterior interosseous nerve (PIN) is at risk of iatrogenic nerve injury during elbow surgery when using a lateral or posterolateral approach. Results of cadaveric studies indicated that maintaining forearm pronation throughout the surgery can help move the PIN away from the surgical window. However, in vivo dynamic migration of the PIN in response to changes in the elbow and forearm position is unclear. This study aimed to clarify the in vivo dynamic migration pattern of the PIN in response to changes in the elbow and forearm position using ultrasound imaging.</p><p><strong>Methods: </strong>This study included 43 upper extremities of 22 healthy volunteers (16 females; mean age, 29 years). Using ultrasound imaging, we measured the shortest distance from the radial head (RH) to the point where the PIN crossed the lateral aspect of the radial axis in six positions of the elbow and forearm: 90° forearm supination, 90° pronation, and neutral forearm position, each at 135° of elbow flexion and 0° of elbow extension.</p><p><strong>Results: </strong>The RH-to-nerve distance was greater during elbow extension than during elbow flexion regardless of the forearm position. However, the maximum migration distance was 3.5 mm when transitioning from elbow extension and forearm pronation (25.1 mm) to elbow flexion and forearm supination (21.6 mm).</p><p><strong>Conclusions: </strong>Although forearm pronation may help move the PIN away from the surgical window, care should be taken not to injure the nerve when performing elbow surgery using a lateral or posterolateral approach. Level of evidence: III.</p>\",\"PeriodicalId\":33981,\"journal\":{\"name\":\"Clinics in Shoulder and Elbow\",\"volume\":\" \",\"pages\":\"407-411\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11615462/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Clinics in Shoulder and Elbow\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.5397/cise.2024.00213\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Clinics in Shoulder and Elbow","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.5397/cise.2024.00213","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/27 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
In vivo dynamic migration of the posterior interosseous nerve across various elbow and forearm positions.
Background: The posterior interosseous nerve (PIN) is at risk of iatrogenic nerve injury during elbow surgery when using a lateral or posterolateral approach. Results of cadaveric studies indicated that maintaining forearm pronation throughout the surgery can help move the PIN away from the surgical window. However, in vivo dynamic migration of the PIN in response to changes in the elbow and forearm position is unclear. This study aimed to clarify the in vivo dynamic migration pattern of the PIN in response to changes in the elbow and forearm position using ultrasound imaging.
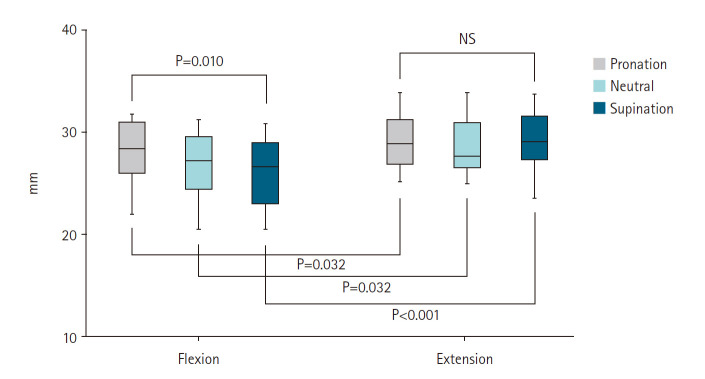
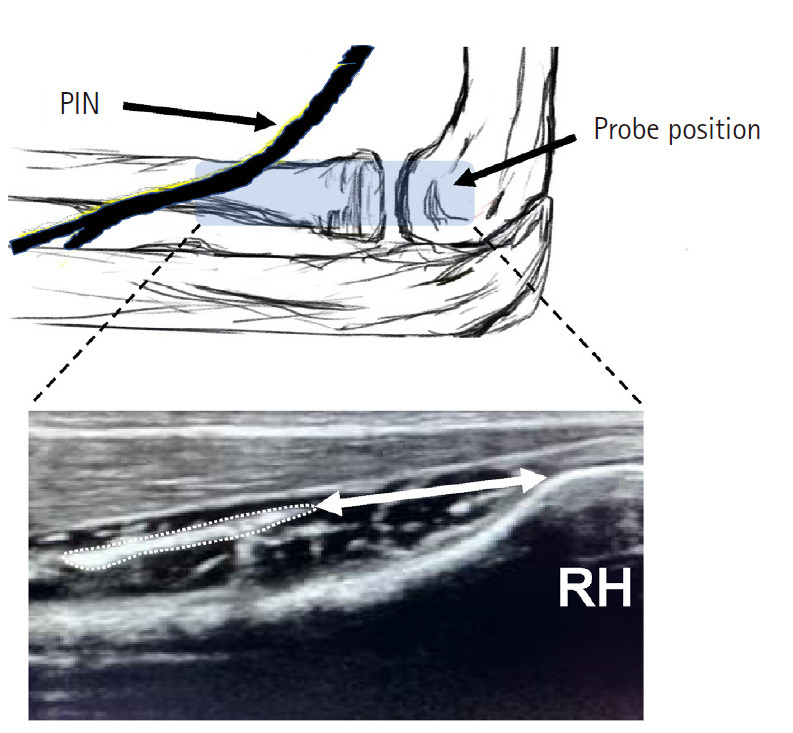
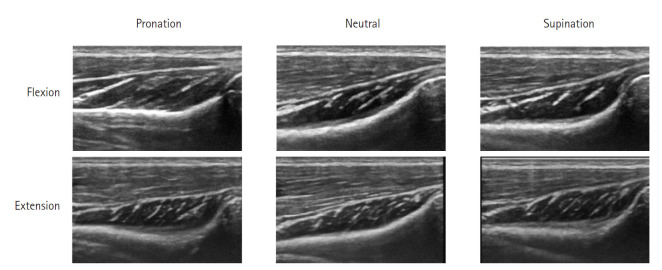
Methods: This study included 43 upper extremities of 22 healthy volunteers (16 females; mean age, 29 years). Using ultrasound imaging, we measured the shortest distance from the radial head (RH) to the point where the PIN crossed the lateral aspect of the radial axis in six positions of the elbow and forearm: 90° forearm supination, 90° pronation, and neutral forearm position, each at 135° of elbow flexion and 0° of elbow extension.
Results: The RH-to-nerve distance was greater during elbow extension than during elbow flexion regardless of the forearm position. However, the maximum migration distance was 3.5 mm when transitioning from elbow extension and forearm pronation (25.1 mm) to elbow flexion and forearm supination (21.6 mm).
Conclusions: Although forearm pronation may help move the PIN away from the surgical window, care should be taken not to injure the nerve when performing elbow surgery using a lateral or posterolateral approach. Level of evidence: III.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


