Diana Marcela Grajales-Urrego, Fabián Mantilla-Sylvain, Mariam Carolina Rolon-Cadena, William Mauricio Basto-Borbón, Johanna Álvarez-Figueroa
{"title":"真菌引起的静脉肠缺血是免疫力低下患者肠梗阻的原因之一:病例报告和文献综述。","authors":"Diana Marcela Grajales-Urrego, Fabián Mantilla-Sylvain, Mariam Carolina Rolon-Cadena, William Mauricio Basto-Borbón, Johanna Álvarez-Figueroa","doi":"10.1186/s13099-024-00658-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Mucormycosis is a highly lethal opportunistic fungal disease caused by ubiquitous molds of the order Mucorales, with Rhizopus, Lichtheimia and Mucor being the most common genera. This rare disease primarily affects immunocompromised patients, with presentations ranging from rhino-orbito-cerebral infections to disseminated mucormycosis with angioinvasion, leading to thrombosis and tissue infarction. Gastrointestinal mucormycosis is the least common clinical presentation and is believed to be secondary to spore ingestion. It can involve multiple components of the gastrointestinal tract, such as the stomach, liver, ileum, and colon, with nonspecific manifestations, including pain, nausea, vomiting, and abdominal distension. The initial clinical presentation may even manifest as gastrointestinal bleeding due to gastric ulceration or intestinal perforation.</p><p><strong>Case presentation: </strong>Here we present the case of a 48-year-old male patient with a 9-year history of human immunodeficiency virus (HIV) infection who was hospitalized in the context of febrile neutropenia and whose acute respiratory infection was documented; therefore, antibiotic treatment was initiated. However, due to persistent febrile peaks and peripheral blood showing documentation of multilineage cytopenias, a bone marrow biopsy was performed, compatible with presenting features of marrow myelodysplasia. During hospitalization, the patient presented left flank abdominal pain, and an abdominal computed tomography (CT) scan revealed signs of intussusception of a small bowel loop at the distal jejunum level, leading to intestinal obstruction with ischemic progression, requiring ileectomy (60 cm). Histopathological analysis of the resected intestine revealed severe transmural ischemic changes associated with venous thrombosis due to fungal structures, with histochemical studies demonstrating the presence of zygomycete (Mucor) fungal structures, leading to the initiation of treatment with amphotericin B. However, despite treatment, the patient experienced progressive clinical deterioration with persistent fever and ventilatory failure, with follow-up tests showing absolute neutropenia and blood cultures positive for yeast, leading to death 52 days after admission.</p><p><strong>Conclusions: </strong>The diagnosis of intestinal mucormycosis may be delayed due to the lack of specificity of the signs and symptoms. Pathologists as well as histopathological studies are essential for timely treatment.</p>","PeriodicalId":12833,"journal":{"name":"Gut Pathogens","volume":"16 1","pages":"66"},"PeriodicalIF":4.0000,"publicationDate":"2024-11-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552342/pdf/","citationCount":"0","resultStr":"{\"title\":\"Venous intestinal ischemia of fungal origin as a cause of intestinal obstruction in immunocompromised patients: case report and literature review.\",\"authors\":\"Diana Marcela Grajales-Urrego, Fabián Mantilla-Sylvain, Mariam Carolina Rolon-Cadena, William Mauricio Basto-Borbón, Johanna Álvarez-Figueroa\",\"doi\":\"10.1186/s13099-024-00658-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Mucormycosis is a highly lethal opportunistic fungal disease caused by ubiquitous molds of the order Mucorales, with Rhizopus, Lichtheimia and Mucor being the most common genera. This rare disease primarily affects immunocompromised patients, with presentations ranging from rhino-orbito-cerebral infections to disseminated mucormycosis with angioinvasion, leading to thrombosis and tissue infarction. Gastrointestinal mucormycosis is the least common clinical presentation and is believed to be secondary to spore ingestion. It can involve multiple components of the gastrointestinal tract, such as the stomach, liver, ileum, and colon, with nonspecific manifestations, including pain, nausea, vomiting, and abdominal distension. The initial clinical presentation may even manifest as gastrointestinal bleeding due to gastric ulceration or intestinal perforation.</p><p><strong>Case presentation: </strong>Here we present the case of a 48-year-old male patient with a 9-year history of human immunodeficiency virus (HIV) infection who was hospitalized in the context of febrile neutropenia and whose acute respiratory infection was documented; therefore, antibiotic treatment was initiated. However, due to persistent febrile peaks and peripheral blood showing documentation of multilineage cytopenias, a bone marrow biopsy was performed, compatible with presenting features of marrow myelodysplasia. During hospitalization, the patient presented left flank abdominal pain, and an abdominal computed tomography (CT) scan revealed signs of intussusception of a small bowel loop at the distal jejunum level, leading to intestinal obstruction with ischemic progression, requiring ileectomy (60 cm). Histopathological analysis of the resected intestine revealed severe transmural ischemic changes associated with venous thrombosis due to fungal structures, with histochemical studies demonstrating the presence of zygomycete (Mucor) fungal structures, leading to the initiation of treatment with amphotericin B. However, despite treatment, the patient experienced progressive clinical deterioration with persistent fever and ventilatory failure, with follow-up tests showing absolute neutropenia and blood cultures positive for yeast, leading to death 52 days after admission.</p><p><strong>Conclusions: </strong>The diagnosis of intestinal mucormycosis may be delayed due to the lack of specificity of the signs and symptoms. Pathologists as well as histopathological studies are essential for timely treatment.</p>\",\"PeriodicalId\":12833,\"journal\":{\"name\":\"Gut Pathogens\",\"volume\":\"16 1\",\"pages\":\"66\"},\"PeriodicalIF\":4.0000,\"publicationDate\":\"2024-11-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552342/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Gut Pathogens\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13099-024-00658-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Gut Pathogens","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13099-024-00658-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
引用次数: 0
摘要
背景:粘孢子菌病是一种高度致命的机会性真菌疾病,由无处不在的粘孢子菌目霉菌引起,其中最常见的菌属是根霉属、李氏霉属和粘孢子属。这种罕见的疾病主要影响免疫力低下的患者,表现形式从鼻-眼-脑感染到播散性粘孢子菌病,并伴有血管侵犯,导致血栓形成和组织梗塞。胃肠道粘液瘤病是最不常见的临床表现,据信是继发于孢子摄入。它可累及胃、肝、回肠和结肠等胃肠道的多个部位,并伴有疼痛、恶心、呕吐和腹胀等非特异性表现。最初的临床表现甚至可能表现为胃溃疡或肠穿孔导致的消化道出血:我们在此介绍一例 48 岁男性患者的病例,该患者有 9 年的人类免疫缺陷病毒(HIV)感染史,因发热性中性粒细胞减少症住院治疗,其急性呼吸道感染记录在案,因此开始了抗生素治疗。然而,由于发热高峰持续存在,且外周血显示多系细胞减少,因此对其进行了骨髓活检,结果显示其骨髓增生异常。住院期间,患者出现左侧腹痛,腹部计算机断层扫描(CT)显示空肠远端有小肠襻肠套叠的迹象,导致肠梗阻和缺血性进展,需要进行回肠切除术(60 厘米)。切除肠道的组织病理学分析显示,真菌结构导致的静脉血栓形成引起了严重的跨膜缺血性病变,组织化学研究显示存在子囊菌(粘孢子菌)真菌结构,因此开始使用两性霉素 B 进行治疗。然而,尽管进行了治疗,患者的临床症状仍在逐渐恶化,出现持续发热和呼吸衰竭,随访检查显示绝对中性粒细胞减少,血培养酵母菌阳性,最终在入院 52 天后死亡:结论:由于症状和体征缺乏特异性,肠粘孢子菌病的诊断可能会被延误。病理学家和组织病理学研究对及时治疗至关重要。
Venous intestinal ischemia of fungal origin as a cause of intestinal obstruction in immunocompromised patients: case report and literature review.
Background: Mucormycosis is a highly lethal opportunistic fungal disease caused by ubiquitous molds of the order Mucorales, with Rhizopus, Lichtheimia and Mucor being the most common genera. This rare disease primarily affects immunocompromised patients, with presentations ranging from rhino-orbito-cerebral infections to disseminated mucormycosis with angioinvasion, leading to thrombosis and tissue infarction. Gastrointestinal mucormycosis is the least common clinical presentation and is believed to be secondary to spore ingestion. It can involve multiple components of the gastrointestinal tract, such as the stomach, liver, ileum, and colon, with nonspecific manifestations, including pain, nausea, vomiting, and abdominal distension. The initial clinical presentation may even manifest as gastrointestinal bleeding due to gastric ulceration or intestinal perforation.
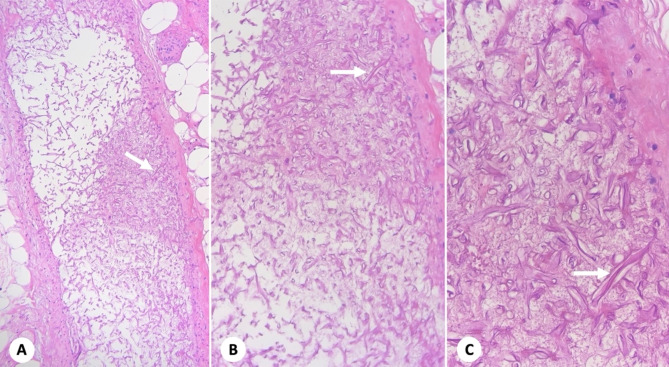
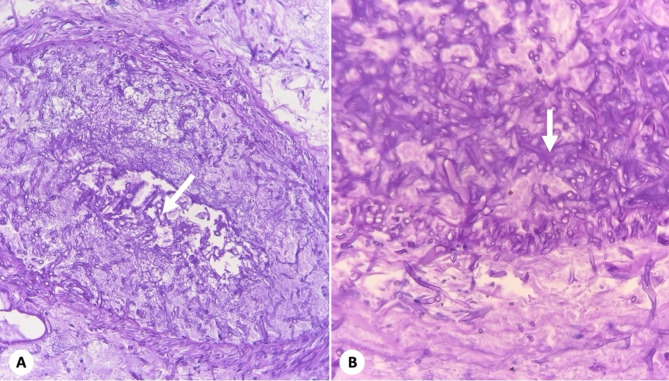
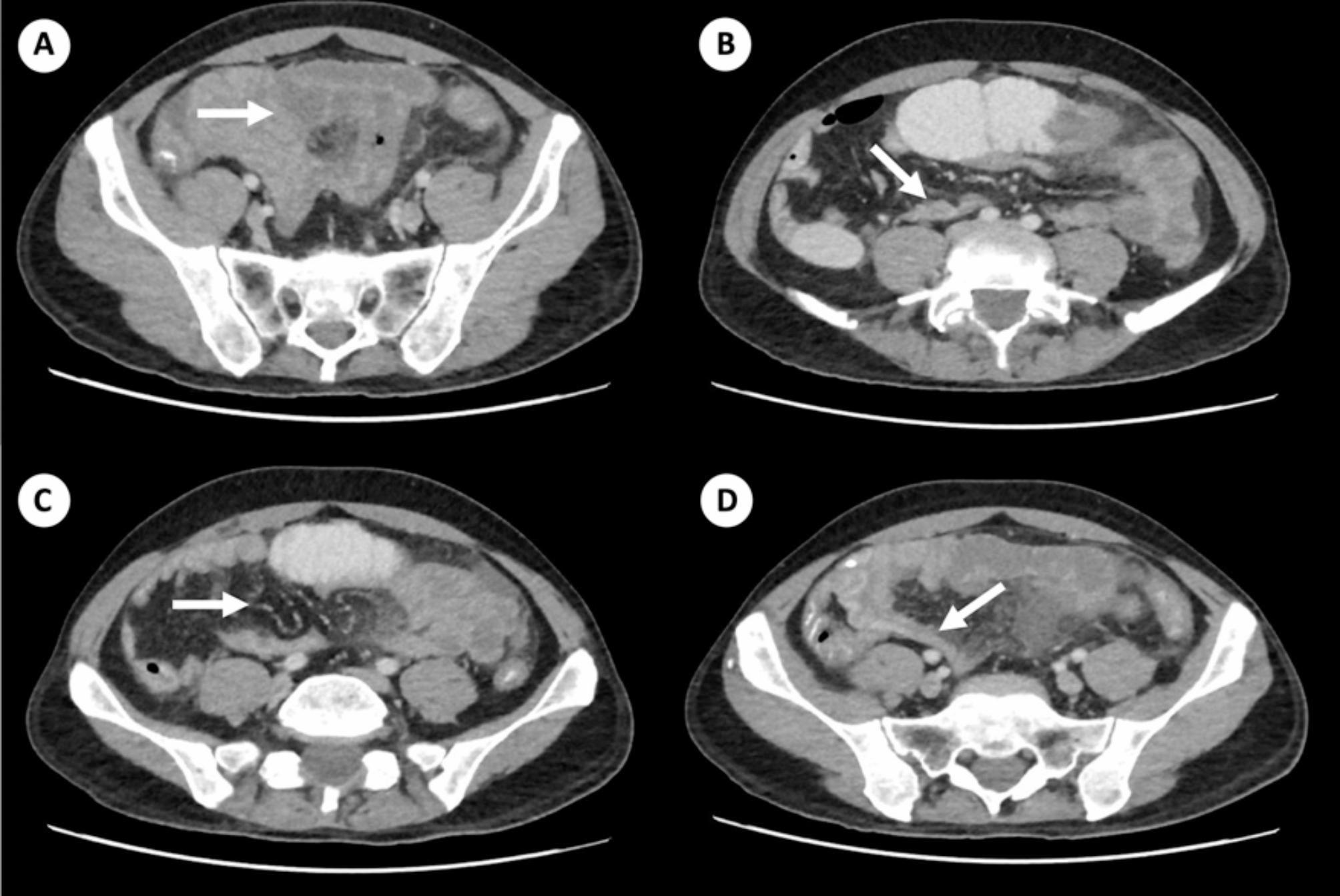
Case presentation: Here we present the case of a 48-year-old male patient with a 9-year history of human immunodeficiency virus (HIV) infection who was hospitalized in the context of febrile neutropenia and whose acute respiratory infection was documented; therefore, antibiotic treatment was initiated. However, due to persistent febrile peaks and peripheral blood showing documentation of multilineage cytopenias, a bone marrow biopsy was performed, compatible with presenting features of marrow myelodysplasia. During hospitalization, the patient presented left flank abdominal pain, and an abdominal computed tomography (CT) scan revealed signs of intussusception of a small bowel loop at the distal jejunum level, leading to intestinal obstruction with ischemic progression, requiring ileectomy (60 cm). Histopathological analysis of the resected intestine revealed severe transmural ischemic changes associated with venous thrombosis due to fungal structures, with histochemical studies demonstrating the presence of zygomycete (Mucor) fungal structures, leading to the initiation of treatment with amphotericin B. However, despite treatment, the patient experienced progressive clinical deterioration with persistent fever and ventilatory failure, with follow-up tests showing absolute neutropenia and blood cultures positive for yeast, leading to death 52 days after admission.
Conclusions: The diagnosis of intestinal mucormycosis may be delayed due to the lack of specificity of the signs and symptoms. Pathologists as well as histopathological studies are essential for timely treatment.
Gut PathogensGASTROENTEROLOGY & HEPATOLOGY-MICROBIOLOGY
CiteScore
7.70
自引率
2.40%
发文量
43
期刊介绍:
Gut Pathogens is a fast publishing, inclusive and prominent international journal which recognizes the need for a publishing platform uniquely tailored to reflect the full breadth of research in the biology and medicine of pathogens, commensals and functional microbiota of the gut. The journal publishes basic, clinical and cutting-edge research on all aspects of the above mentioned organisms including probiotic bacteria and yeasts and their products. The scope also covers the related ecology, molecular genetics, physiology and epidemiology of these microbes. The journal actively invites timely reports on the novel aspects of genomics, metagenomics, microbiota profiling and systems biology.
Gut Pathogens will also consider, at the discretion of the editors, descriptive studies identifying a new genome sequence of a gut microbe or a series of related microbes (such as those obtained from new hosts, niches, settings, outbreaks and epidemics) and those obtained from single or multiple hosts at one or different time points (chronological evolution).
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


