Wout Willem Antoon van den Broek, Jaouad Azzahhafi, Dean R P P Chan Pin Yin, Niels M R van der Sangen, Shabiga Sivanesan, Lea M Dijksman, Ronald J Walhout, Melvyn Tjon Joe Gin, Nicoline J Breet, Jorina Langerveld, Georgios J Vlachojannis, Rutger J van Bommel, Yolande Appelman, Ron H N van Schaik, José P S Henriques, Wouter J Kikkert, Jurriën M Ten Berg
{"title":"对急性冠状动脉综合征患者实施基因型指导下的去梗策略的成本效益。","authors":"Wout Willem Antoon van den Broek, Jaouad Azzahhafi, Dean R P P Chan Pin Yin, Niels M R van der Sangen, Shabiga Sivanesan, Lea M Dijksman, Ronald J Walhout, Melvyn Tjon Joe Gin, Nicoline J Breet, Jorina Langerveld, Georgios J Vlachojannis, Rutger J van Bommel, Yolande Appelman, Ron H N van Schaik, José P S Henriques, Wouter J Kikkert, Jurriën M Ten Berg","doi":"10.1093/ehjcvp/pvae087","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>A genotype-guided P2Y12-inhibitor de-escalation strategy, switching acute coronary syndrome (ACS) patients without a CYP2C19 loss-of-function allele from ticagrelor or prasugrel to clopidogrel, has shown to reduce bleeding risk without affecting the effectivity of therapy by increasing ischaemic risk. We estimated the cost-effectiveness of this personalized approach compared to standard dual antiplatelet therapy (DAPT; aspirin plus ticagrelor/prasugrel) in the Netherlands.</p><p><strong>Methods and results: </strong>We developed a 1-year decision tree based on results of the FORCE-ACS registry, comparing a cohort of ACS patients who underwent genotyping with a cohort of ACS patients treated with standard DAPT. This was followed by a lifelong Markov model to compare lifetime costs and quality-adjusted life years (QALYs) for a fictional cohort of 1000 patients. The cost-effectiveness analysis was performed from the perspective of the Dutch healthcare system. A genotype-guided de-escalation strategy led to an increase of 57.73 QALYs and saved €808788 compared to standard DAPT based on a lifetime horizon. Probabilistic sensitivity analysis showed that the genotype-guided strategy was cost-saving in 96% and increased QALYs in 87% of simulations. The intervention remained cost-effective in the scenario where prices for all P2Y12 inhibitors were equalized. The genotype-guided strategy remained dominant in various other scenarios and sensitivity analyses.</p><p><strong>Conclusion: </strong>A genotype-guided de-escalation strategy in patients with ACS was both cost-saving and yielded higher QALYs compared to standard DAPT, highlighting its potential for implementation in clinical practice. Trial registration: ClinicalTrials.gov identifier: NCT03823547.</p>","PeriodicalId":11982,"journal":{"name":"European Heart Journal - Cardiovascular Pharmacotherapy","volume":" ","pages":"230-240"},"PeriodicalIF":6.1000,"publicationDate":"2025-05-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12046577/pdf/","citationCount":"0","resultStr":"{\"title\":\"Cost-effectiveness of implementing a genotype-guided de-escalation strategy in patients with acute coronary syndrome.\",\"authors\":\"Wout Willem Antoon van den Broek, Jaouad Azzahhafi, Dean R P P Chan Pin Yin, Niels M R van der Sangen, Shabiga Sivanesan, Lea M Dijksman, Ronald J Walhout, Melvyn Tjon Joe Gin, Nicoline J Breet, Jorina Langerveld, Georgios J Vlachojannis, Rutger J van Bommel, Yolande Appelman, Ron H N van Schaik, José P S Henriques, Wouter J Kikkert, Jurriën M Ten Berg\",\"doi\":\"10.1093/ehjcvp/pvae087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>A genotype-guided P2Y12-inhibitor de-escalation strategy, switching acute coronary syndrome (ACS) patients without a CYP2C19 loss-of-function allele from ticagrelor or prasugrel to clopidogrel, has shown to reduce bleeding risk without affecting the effectivity of therapy by increasing ischaemic risk. We estimated the cost-effectiveness of this personalized approach compared to standard dual antiplatelet therapy (DAPT; aspirin plus ticagrelor/prasugrel) in the Netherlands.</p><p><strong>Methods and results: </strong>We developed a 1-year decision tree based on results of the FORCE-ACS registry, comparing a cohort of ACS patients who underwent genotyping with a cohort of ACS patients treated with standard DAPT. This was followed by a lifelong Markov model to compare lifetime costs and quality-adjusted life years (QALYs) for a fictional cohort of 1000 patients. The cost-effectiveness analysis was performed from the perspective of the Dutch healthcare system. A genotype-guided de-escalation strategy led to an increase of 57.73 QALYs and saved €808788 compared to standard DAPT based on a lifetime horizon. Probabilistic sensitivity analysis showed that the genotype-guided strategy was cost-saving in 96% and increased QALYs in 87% of simulations. The intervention remained cost-effective in the scenario where prices for all P2Y12 inhibitors were equalized. The genotype-guided strategy remained dominant in various other scenarios and sensitivity analyses.</p><p><strong>Conclusion: </strong>A genotype-guided de-escalation strategy in patients with ACS was both cost-saving and yielded higher QALYs compared to standard DAPT, highlighting its potential for implementation in clinical practice. Trial registration: ClinicalTrials.gov identifier: NCT03823547.</p>\",\"PeriodicalId\":11982,\"journal\":{\"name\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"volume\":\" \",\"pages\":\"230-240\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2025-05-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC12046577/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcvp/pvae087\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvae087","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Cost-effectiveness of implementing a genotype-guided de-escalation strategy in patients with acute coronary syndrome.
Aims: A genotype-guided P2Y12-inhibitor de-escalation strategy, switching acute coronary syndrome (ACS) patients without a CYP2C19 loss-of-function allele from ticagrelor or prasugrel to clopidogrel, has shown to reduce bleeding risk without affecting the effectivity of therapy by increasing ischaemic risk. We estimated the cost-effectiveness of this personalized approach compared to standard dual antiplatelet therapy (DAPT; aspirin plus ticagrelor/prasugrel) in the Netherlands.
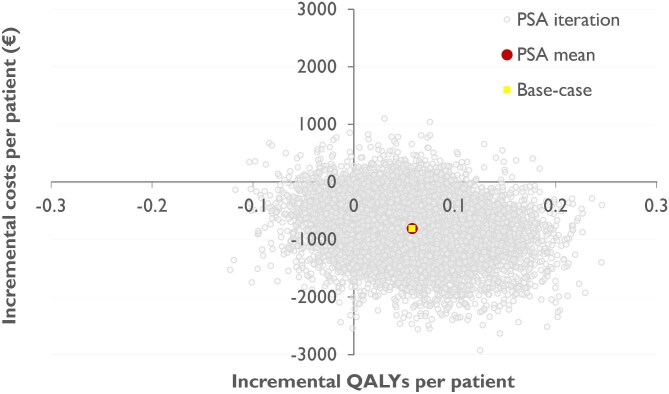
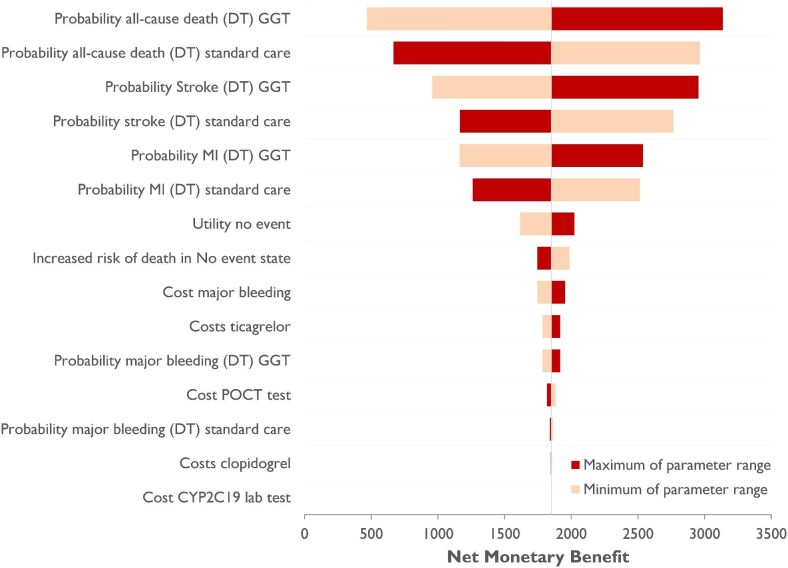
Methods and results: We developed a 1-year decision tree based on results of the FORCE-ACS registry, comparing a cohort of ACS patients who underwent genotyping with a cohort of ACS patients treated with standard DAPT. This was followed by a lifelong Markov model to compare lifetime costs and quality-adjusted life years (QALYs) for a fictional cohort of 1000 patients. The cost-effectiveness analysis was performed from the perspective of the Dutch healthcare system. A genotype-guided de-escalation strategy led to an increase of 57.73 QALYs and saved €808788 compared to standard DAPT based on a lifetime horizon. Probabilistic sensitivity analysis showed that the genotype-guided strategy was cost-saving in 96% and increased QALYs in 87% of simulations. The intervention remained cost-effective in the scenario where prices for all P2Y12 inhibitors were equalized. The genotype-guided strategy remained dominant in various other scenarios and sensitivity analyses.
Conclusion: A genotype-guided de-escalation strategy in patients with ACS was both cost-saving and yielded higher QALYs compared to standard DAPT, highlighting its potential for implementation in clinical practice. Trial registration: ClinicalTrials.gov identifier: NCT03823547.
期刊介绍:
The European Heart Journal - Cardiovascular Pharmacotherapy (EHJ-CVP) is an international, peer-reviewed journal published in English, specifically dedicated to clinical cardiovascular pharmacology. EHJ-CVP publishes original articles focusing on clinical research involving both new and established drugs and methods, along with meta-analyses and topical reviews. The journal's primary aim is to enhance the pharmacological treatment of patients with cardiovascular disease by interpreting and integrating new scientific developments in this field.
While the emphasis is on clinical topics, EHJ-CVP also considers basic research articles from fields such as physiology and molecular biology that contribute to the understanding of cardiovascular drug therapy. These may include articles related to new drug development and evaluation, the physiological and pharmacological basis of drug action, metabolism, drug interactions, and side effects.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


