Gurleen Sahi, Jennifer Reid, Louise Moist, Michael Chiu, Amanda Vinson, Saverio Stranges, Kyla Naylor, Yunxu Zhu, Kristin K Clemens
{"title":"高体重指数肾病患者的患病率、特征和预后:一项基于人群的队列研究。","authors":"Gurleen Sahi, Jennifer Reid, Louise Moist, Michael Chiu, Amanda Vinson, Saverio Stranges, Kyla Naylor, Yunxu Zhu, Kristin K Clemens","doi":"10.1177/20543581241293199","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Obesity has a major impact on health and health care, particularly in those with chronic kidney disease (CKD).</p><p><strong>Objective: </strong>The objective was to describe the prevalence, characteristics, and outcomes of people living with CKD and obesity (defined by a body mass index [BMI] ≥30 kg/m<sup>2</sup>) in Canada.</p><p><strong>Design: </strong>Population-based cohort study using linked administrative health data (ICES).</p><p><strong>Patients: </strong>Adults aged 18 year and older with CKD G1-5D who had a height and weight recorded during a visit to an academic hospital in London Ontario Canada, between January 2010 and December 2019.</p><p><strong>Measures: </strong>CKD as defined by CKD 3A or higher. BMI as defined by weight kg/m<sup>2</sup>.</p><p><strong>Methods: </strong>As a primary interest, we described the percentage of patients with CKD across different BMI categories (<25 kg/m<sup>2</sup>, BMI 25-29.9 kg/m<sup>2</sup>, and BMI ≥30 kg/m<sup>2</sup>), as well as their demographic and clinical profiles. As secondary interests, we followed patients until January 1, 2022 to summarize: (1) the percentage with CKD G3 who had kidney disease progression (50% decline from baseline estimated glomerular filtration rate [eGFR]) by BMI category, (2) the percentage with CKD G3-4 who developed kidney failure (initiation of maintenance dialysis or an eGFR of <15 mL/min/1.73 m<sup>2</sup>) by BMI category, (3) the percentage with CKD G4-G5D who received a kidney transplant by BMI category, and (4) post-transplant outcomes in those transplanted over the study period, by BMI category. We performed similar analyses across CKD risk categories.</p><p><strong>Results: </strong>Of the 198 151 patients included, the percentage with obesity defined by a BMI ≥30 kg/m<sup>2</sup> increased from CKD G1 to CKD G4 (ie, 37% of those with CKD G1 had a BMI ≥30 kg/m<sup>2</sup> vs 40.9% of CKD G4). In CKD G5D and CKD T, the prevalence of high BMI appeared to drop (only ~38% had a BMI ≥30 kg/m<sup>2</sup> across groups). Across CKD categories, those with a BMI ≥30 kg/m<sup>2</sup> appeared to have more comorbidities, use more health care resources, and have more socioeconomic disparities than those with lower BMIs. Although secondary outcome events were limited, those with G3-4 with a BMI ≥30 kg/m<sup>2</sup> appeared to have a higher risk of CKD progression and those with CKD G5D with BMI ≥30 kg/m<sup>2</sup> were less likely to receive transplant over the study period. Interestingly those transplanted with a BMI ≥30 kg/m<sup>2</sup> appeared to have fewer post-transplant complications. We also observed an \"obesity-paradox\" in the risk of mortality, with high BMI appearing protective, particularly in the end stages of kidney disease.</p><p><strong>Limitations: </strong>We used BMI to capture obesity in this study but recognize its limitations as a measure of body composition. Secondary outcomes were descriptive and unadjusted due to small sample size and may have been subject to selection bias and confounding.</p><p><strong>Conclusions: </strong>Obesity defined by high BMI is highly prevalent in people with CKD, and patients have health, health care, and social disparity. Future studies to understand the impact of BMI on patients with CKD and how to individualize and manage BMI and obesity across the spectrum of CKD remain important.</p>","PeriodicalId":9426,"journal":{"name":"Canadian Journal of Kidney Health and Disease","volume":"11 ","pages":"20543581241293199"},"PeriodicalIF":1.5000,"publicationDate":"2024-11-10","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552050/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prevalence, Characteristics, and Outcomes of People With A High Body Mass Index Across the Kidney Disease Spectrum: A Population-Based Cohort Study.\",\"authors\":\"Gurleen Sahi, Jennifer Reid, Louise Moist, Michael Chiu, Amanda Vinson, Saverio Stranges, Kyla Naylor, Yunxu Zhu, Kristin K Clemens\",\"doi\":\"10.1177/20543581241293199\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Obesity has a major impact on health and health care, particularly in those with chronic kidney disease (CKD).</p><p><strong>Objective: </strong>The objective was to describe the prevalence, characteristics, and outcomes of people living with CKD and obesity (defined by a body mass index [BMI] ≥30 kg/m<sup>2</sup>) in Canada.</p><p><strong>Design: </strong>Population-based cohort study using linked administrative health data (ICES).</p><p><strong>Patients: </strong>Adults aged 18 year and older with CKD G1-5D who had a height and weight recorded during a visit to an academic hospital in London Ontario Canada, between January 2010 and December 2019.</p><p><strong>Measures: </strong>CKD as defined by CKD 3A or higher. BMI as defined by weight kg/m<sup>2</sup>.</p><p><strong>Methods: </strong>As a primary interest, we described the percentage of patients with CKD across different BMI categories (<25 kg/m<sup>2</sup>, BMI 25-29.9 kg/m<sup>2</sup>, and BMI ≥30 kg/m<sup>2</sup>), as well as their demographic and clinical profiles. As secondary interests, we followed patients until January 1, 2022 to summarize: (1) the percentage with CKD G3 who had kidney disease progression (50% decline from baseline estimated glomerular filtration rate [eGFR]) by BMI category, (2) the percentage with CKD G3-4 who developed kidney failure (initiation of maintenance dialysis or an eGFR of <15 mL/min/1.73 m<sup>2</sup>) by BMI category, (3) the percentage with CKD G4-G5D who received a kidney transplant by BMI category, and (4) post-transplant outcomes in those transplanted over the study period, by BMI category. We performed similar analyses across CKD risk categories.</p><p><strong>Results: </strong>Of the 198 151 patients included, the percentage with obesity defined by a BMI ≥30 kg/m<sup>2</sup> increased from CKD G1 to CKD G4 (ie, 37% of those with CKD G1 had a BMI ≥30 kg/m<sup>2</sup> vs 40.9% of CKD G4). In CKD G5D and CKD T, the prevalence of high BMI appeared to drop (only ~38% had a BMI ≥30 kg/m<sup>2</sup> across groups). Across CKD categories, those with a BMI ≥30 kg/m<sup>2</sup> appeared to have more comorbidities, use more health care resources, and have more socioeconomic disparities than those with lower BMIs. Although secondary outcome events were limited, those with G3-4 with a BMI ≥30 kg/m<sup>2</sup> appeared to have a higher risk of CKD progression and those with CKD G5D with BMI ≥30 kg/m<sup>2</sup> were less likely to receive transplant over the study period. Interestingly those transplanted with a BMI ≥30 kg/m<sup>2</sup> appeared to have fewer post-transplant complications. We also observed an \\\"obesity-paradox\\\" in the risk of mortality, with high BMI appearing protective, particularly in the end stages of kidney disease.</p><p><strong>Limitations: </strong>We used BMI to capture obesity in this study but recognize its limitations as a measure of body composition. Secondary outcomes were descriptive and unadjusted due to small sample size and may have been subject to selection bias and confounding.</p><p><strong>Conclusions: </strong>Obesity defined by high BMI is highly prevalent in people with CKD, and patients have health, health care, and social disparity. Future studies to understand the impact of BMI on patients with CKD and how to individualize and manage BMI and obesity across the spectrum of CKD remain important.</p>\",\"PeriodicalId\":9426,\"journal\":{\"name\":\"Canadian Journal of Kidney Health and Disease\",\"volume\":\"11 \",\"pages\":\"20543581241293199\"},\"PeriodicalIF\":1.5000,\"publicationDate\":\"2024-11-10\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11552050/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Canadian Journal of Kidney Health and Disease\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/20543581241293199\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Canadian Journal of Kidney Health and Disease","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/20543581241293199","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Prevalence, Characteristics, and Outcomes of People With A High Body Mass Index Across the Kidney Disease Spectrum: A Population-Based Cohort Study.
Background: Obesity has a major impact on health and health care, particularly in those with chronic kidney disease (CKD).
Objective: The objective was to describe the prevalence, characteristics, and outcomes of people living with CKD and obesity (defined by a body mass index [BMI] ≥30 kg/m2) in Canada.
Design: Population-based cohort study using linked administrative health data (ICES).
Patients: Adults aged 18 year and older with CKD G1-5D who had a height and weight recorded during a visit to an academic hospital in London Ontario Canada, between January 2010 and December 2019.
Measures: CKD as defined by CKD 3A or higher. BMI as defined by weight kg/m2.
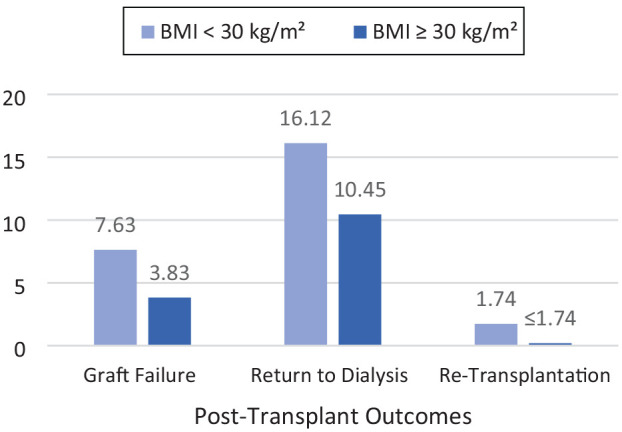
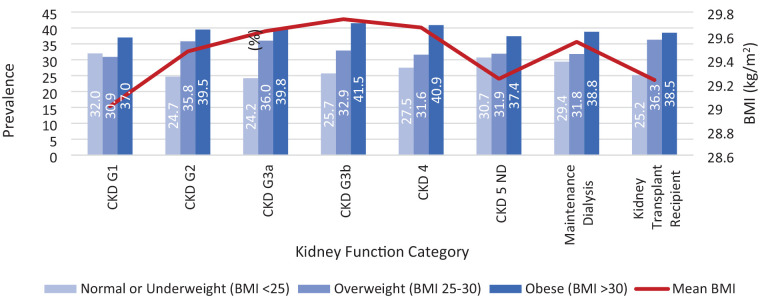
Methods: As a primary interest, we described the percentage of patients with CKD across different BMI categories (<25 kg/m2, BMI 25-29.9 kg/m2, and BMI ≥30 kg/m2), as well as their demographic and clinical profiles. As secondary interests, we followed patients until January 1, 2022 to summarize: (1) the percentage with CKD G3 who had kidney disease progression (50% decline from baseline estimated glomerular filtration rate [eGFR]) by BMI category, (2) the percentage with CKD G3-4 who developed kidney failure (initiation of maintenance dialysis or an eGFR of <15 mL/min/1.73 m2) by BMI category, (3) the percentage with CKD G4-G5D who received a kidney transplant by BMI category, and (4) post-transplant outcomes in those transplanted over the study period, by BMI category. We performed similar analyses across CKD risk categories.
Results: Of the 198 151 patients included, the percentage with obesity defined by a BMI ≥30 kg/m2 increased from CKD G1 to CKD G4 (ie, 37% of those with CKD G1 had a BMI ≥30 kg/m2 vs 40.9% of CKD G4). In CKD G5D and CKD T, the prevalence of high BMI appeared to drop (only ~38% had a BMI ≥30 kg/m2 across groups). Across CKD categories, those with a BMI ≥30 kg/m2 appeared to have more comorbidities, use more health care resources, and have more socioeconomic disparities than those with lower BMIs. Although secondary outcome events were limited, those with G3-4 with a BMI ≥30 kg/m2 appeared to have a higher risk of CKD progression and those with CKD G5D with BMI ≥30 kg/m2 were less likely to receive transplant over the study period. Interestingly those transplanted with a BMI ≥30 kg/m2 appeared to have fewer post-transplant complications. We also observed an "obesity-paradox" in the risk of mortality, with high BMI appearing protective, particularly in the end stages of kidney disease.
Limitations: We used BMI to capture obesity in this study but recognize its limitations as a measure of body composition. Secondary outcomes were descriptive and unadjusted due to small sample size and may have been subject to selection bias and confounding.
Conclusions: Obesity defined by high BMI is highly prevalent in people with CKD, and patients have health, health care, and social disparity. Future studies to understand the impact of BMI on patients with CKD and how to individualize and manage BMI and obesity across the spectrum of CKD remain important.
期刊介绍:
Canadian Journal of Kidney Health and Disease, the official journal of the Canadian Society of Nephrology, is an open access, peer-reviewed online journal that encourages high quality submissions focused on clinical, translational and health services delivery research in the field of chronic kidney disease, dialysis, kidney transplantation and organ donation. Our mandate is to promote and advocate for kidney health as it impacts national and international communities. Basic science, translational studies and clinical studies will be peer reviewed and processed by an Editorial Board comprised of geographically diverse Canadian and international nephrologists, internists and allied health professionals; this Editorial Board is mandated to ensure highest quality publications.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


