{"title":"流动血流动力学评估是否足以降低心力衰竭患者的全因死亡率?","authors":"Reza Tabrizchi","doi":"10.36628/ijhf.2024.0021","DOIUrl":null,"url":null,"abstract":"<p><p>Heart failure (HF) as a syndrome which is <i>normally</i> associated with significant reduction of cardiac output has evolved to include conditions such those of moderate and preserved ejection fraction. While the prevalence of HF in the population is increasing, it is not HF with reduced ejection fraction that is driving the trajectory upward for mortality. There is some evidence to suggest that a better understanding of the pathophysiology, novel pharmacological strategies, devices, as well as remote monitoring of the hemodynamics seem to account for a reduction in the cardiovascular mortality and re-hospitalization in some cohorts with HF. However, the all-cause mortality associated with HF has not been reduced significantly by the current interventions. To explore the potential approaches needed for the strategies and avenues to reduce all-cause mortality in patients with HF, it would be helpful to evaluate the evidence in the literature directed at the care of patients with chronic/acute decompensated HF. It is evident that ambulatory measurements of pressures and volume are pivotal in a better management of HF but unless the interventions extend to an improvement in the renal function, the chances of reducing all-cause mortality seems modest. Therefore, future directions of interventions must not only be directed at close monitoring of pressures and volume simultaneously in HF patients but also at improving renal function. Moreover, it is clear that venous congestion plays a detrimental role in the deterioration of renal function and until measures are in place to reduce it, all-cause mortality will not decrease.</p>","PeriodicalId":101410,"journal":{"name":"International journal of heart failure","volume":"6 4","pages":"149-158"},"PeriodicalIF":0.0000,"publicationDate":"2024-10-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11538721/pdf/","citationCount":"0","resultStr":"{\"title\":\"Adequacy of Ambulatory Hemodynamic Assessments for Reducing All-Cause Mortality in Individuals With Heart Failure.\",\"authors\":\"Reza Tabrizchi\",\"doi\":\"10.36628/ijhf.2024.0021\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Heart failure (HF) as a syndrome which is <i>normally</i> associated with significant reduction of cardiac output has evolved to include conditions such those of moderate and preserved ejection fraction. While the prevalence of HF in the population is increasing, it is not HF with reduced ejection fraction that is driving the trajectory upward for mortality. There is some evidence to suggest that a better understanding of the pathophysiology, novel pharmacological strategies, devices, as well as remote monitoring of the hemodynamics seem to account for a reduction in the cardiovascular mortality and re-hospitalization in some cohorts with HF. However, the all-cause mortality associated with HF has not been reduced significantly by the current interventions. To explore the potential approaches needed for the strategies and avenues to reduce all-cause mortality in patients with HF, it would be helpful to evaluate the evidence in the literature directed at the care of patients with chronic/acute decompensated HF. It is evident that ambulatory measurements of pressures and volume are pivotal in a better management of HF but unless the interventions extend to an improvement in the renal function, the chances of reducing all-cause mortality seems modest. Therefore, future directions of interventions must not only be directed at close monitoring of pressures and volume simultaneously in HF patients but also at improving renal function. Moreover, it is clear that venous congestion plays a detrimental role in the deterioration of renal function and until measures are in place to reduce it, all-cause mortality will not decrease.</p>\",\"PeriodicalId\":101410,\"journal\":{\"name\":\"International journal of heart failure\",\"volume\":\"6 4\",\"pages\":\"149-158\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-10-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11538721/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"International journal of heart failure\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.36628/ijhf.2024.0021\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"International journal of heart failure","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.36628/ijhf.2024.0021","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Adequacy of Ambulatory Hemodynamic Assessments for Reducing All-Cause Mortality in Individuals With Heart Failure.
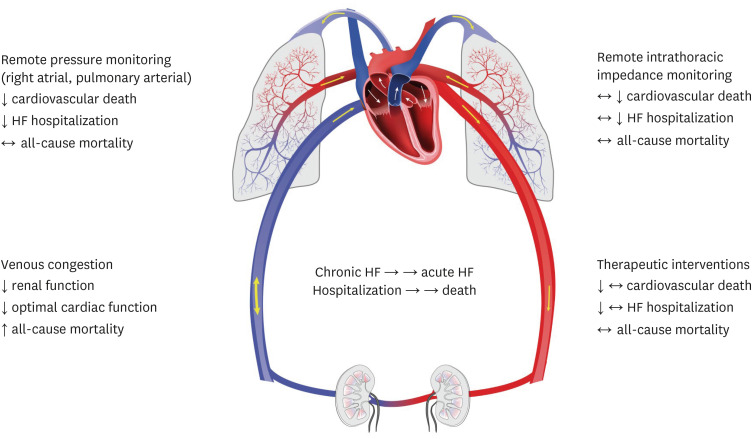
Heart failure (HF) as a syndrome which is normally associated with significant reduction of cardiac output has evolved to include conditions such those of moderate and preserved ejection fraction. While the prevalence of HF in the population is increasing, it is not HF with reduced ejection fraction that is driving the trajectory upward for mortality. There is some evidence to suggest that a better understanding of the pathophysiology, novel pharmacological strategies, devices, as well as remote monitoring of the hemodynamics seem to account for a reduction in the cardiovascular mortality and re-hospitalization in some cohorts with HF. However, the all-cause mortality associated with HF has not been reduced significantly by the current interventions. To explore the potential approaches needed for the strategies and avenues to reduce all-cause mortality in patients with HF, it would be helpful to evaluate the evidence in the literature directed at the care of patients with chronic/acute decompensated HF. It is evident that ambulatory measurements of pressures and volume are pivotal in a better management of HF but unless the interventions extend to an improvement in the renal function, the chances of reducing all-cause mortality seems modest. Therefore, future directions of interventions must not only be directed at close monitoring of pressures and volume simultaneously in HF patients but also at improving renal function. Moreover, it is clear that venous congestion plays a detrimental role in the deterioration of renal function and until measures are in place to reduce it, all-cause mortality will not decrease.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


