Sean R. Miller, Matthew Schipper, Lars G. Fritsche, Ralph Jiang, Garth Strohbehn, Erkin Ötleş, Benjamin H. McMahon, Silvia Crivelli, Rafael Zamora-Resendiz, Nithya Ramnath, Shinjae Yoo, Xin Dai, Kamya Sankar, Donna M. Edwards, Steven G. Allen, Michael D. Green, Alex K. Bryant
{"title":"免疫检查点抑制剂对全国医疗保健系统中泛癌症生存率的影响。","authors":"Sean R. Miller, Matthew Schipper, Lars G. Fritsche, Ralph Jiang, Garth Strohbehn, Erkin Ötleş, Benjamin H. McMahon, Silvia Crivelli, Rafael Zamora-Resendiz, Nithya Ramnath, Shinjae Yoo, Xin Dai, Kamya Sankar, Donna M. Edwards, Steven G. Allen, Michael D. Green, Alex K. Bryant","doi":"10.1002/cam4.70379","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>The cumulative, health system-wide survival benefit of immune checkpoint inhibitors (ICIs) is unclear, particularly among real-world patients with limited life expectancies and among subgroups poorly represented on clinical trials. We sought to determine the health system-wide survival impact of ICIs.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>We identified all patients receiving PD-1/PD-L1 or CTLA-4 inhibitors from 2010 to 2023 in the national Veterans Health Administration (VHA) system (ICI cohort) and all patients who received non-ICI systemic therapy in the years before ICI approval (historical control). ICI and historical control cohorts were matched on multiple cancer-related prognostic factors, comorbidities, and demographics. The effect of ICI on overall survival was quantified with Cox regression incorporating matching weights. Cumulative life-years gained system-wide were calculated from the difference in adjusted 5-year restricted mean survival times.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>There were 27,322 patients in the ICI cohort and 69,801 patients in the historical control cohort. Among ICI patients, the most common cancer types were NSCLC (46%) and melanoma (10%). ICI demonstrated a large OS benefit in most cancer types with heterogeneity across cancer types (NSCLC: adjusted HR [aHR] 0.56, 95% confidence interval [CI] 0.54–0.58, <i>p</i> < 0.001; urothelial: aHR 0.91, 95% CI 0.83–1.01, <i>p</i> = 0.066). The relative benefit of ICI was stable across patient age, comorbidity, and self-reported race subgroups. Across VHA, 15,859 life-years gained were attributable to ICI within 5-years of treatment, with NSCLC contributing the most life-years gained.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>We demonstrated substantial increase in survival due to ICIs across a national health system, including in patient subgroups poorly represented on clinical trials.</p>\n </section>\n </div>","PeriodicalId":139,"journal":{"name":"Cancer Medicine","volume":"13 21","pages":""},"PeriodicalIF":2.9000,"publicationDate":"2024-11-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11541111/pdf/","citationCount":"0","resultStr":"{\"title\":\"Pan-Cancer Survival Impact of Immune Checkpoint Inhibitors in a National Healthcare System\",\"authors\":\"Sean R. Miller, Matthew Schipper, Lars G. Fritsche, Ralph Jiang, Garth Strohbehn, Erkin Ötleş, Benjamin H. McMahon, Silvia Crivelli, Rafael Zamora-Resendiz, Nithya Ramnath, Shinjae Yoo, Xin Dai, Kamya Sankar, Donna M. Edwards, Steven G. Allen, Michael D. Green, Alex K. Bryant\",\"doi\":\"10.1002/cam4.70379\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>The cumulative, health system-wide survival benefit of immune checkpoint inhibitors (ICIs) is unclear, particularly among real-world patients with limited life expectancies and among subgroups poorly represented on clinical trials. We sought to determine the health system-wide survival impact of ICIs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>We identified all patients receiving PD-1/PD-L1 or CTLA-4 inhibitors from 2010 to 2023 in the national Veterans Health Administration (VHA) system (ICI cohort) and all patients who received non-ICI systemic therapy in the years before ICI approval (historical control). ICI and historical control cohorts were matched on multiple cancer-related prognostic factors, comorbidities, and demographics. The effect of ICI on overall survival was quantified with Cox regression incorporating matching weights. Cumulative life-years gained system-wide were calculated from the difference in adjusted 5-year restricted mean survival times.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>There were 27,322 patients in the ICI cohort and 69,801 patients in the historical control cohort. Among ICI patients, the most common cancer types were NSCLC (46%) and melanoma (10%). ICI demonstrated a large OS benefit in most cancer types with heterogeneity across cancer types (NSCLC: adjusted HR [aHR] 0.56, 95% confidence interval [CI] 0.54–0.58, <i>p</i> < 0.001; urothelial: aHR 0.91, 95% CI 0.83–1.01, <i>p</i> = 0.066). The relative benefit of ICI was stable across patient age, comorbidity, and self-reported race subgroups. Across VHA, 15,859 life-years gained were attributable to ICI within 5-years of treatment, with NSCLC contributing the most life-years gained.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>We demonstrated substantial increase in survival due to ICIs across a national health system, including in patient subgroups poorly represented on clinical trials.</p>\\n </section>\\n </div>\",\"PeriodicalId\":139,\"journal\":{\"name\":\"Cancer Medicine\",\"volume\":\"13 21\",\"pages\":\"\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11541111/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cancer Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70379\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ONCOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cancer Medicine","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/cam4.70379","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ONCOLOGY","Score":null,"Total":0}
Pan-Cancer Survival Impact of Immune Checkpoint Inhibitors in a National Healthcare System
Background
The cumulative, health system-wide survival benefit of immune checkpoint inhibitors (ICIs) is unclear, particularly among real-world patients with limited life expectancies and among subgroups poorly represented on clinical trials. We sought to determine the health system-wide survival impact of ICIs.
Methods
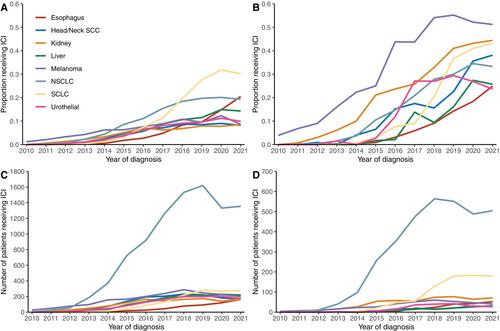
We identified all patients receiving PD-1/PD-L1 or CTLA-4 inhibitors from 2010 to 2023 in the national Veterans Health Administration (VHA) system (ICI cohort) and all patients who received non-ICI systemic therapy in the years before ICI approval (historical control). ICI and historical control cohorts were matched on multiple cancer-related prognostic factors, comorbidities, and demographics. The effect of ICI on overall survival was quantified with Cox regression incorporating matching weights. Cumulative life-years gained system-wide were calculated from the difference in adjusted 5-year restricted mean survival times.
Results
There were 27,322 patients in the ICI cohort and 69,801 patients in the historical control cohort. Among ICI patients, the most common cancer types were NSCLC (46%) and melanoma (10%). ICI demonstrated a large OS benefit in most cancer types with heterogeneity across cancer types (NSCLC: adjusted HR [aHR] 0.56, 95% confidence interval [CI] 0.54–0.58, p < 0.001; urothelial: aHR 0.91, 95% CI 0.83–1.01, p = 0.066). The relative benefit of ICI was stable across patient age, comorbidity, and self-reported race subgroups. Across VHA, 15,859 life-years gained were attributable to ICI within 5-years of treatment, with NSCLC contributing the most life-years gained.
Conclusion
We demonstrated substantial increase in survival due to ICIs across a national health system, including in patient subgroups poorly represented on clinical trials.
期刊介绍:
Cancer Medicine is a peer-reviewed, open access, interdisciplinary journal providing rapid publication of research from global biomedical researchers across the cancer sciences. The journal will consider submissions from all oncologic specialties, including, but not limited to, the following areas:
Clinical Cancer Research
Translational research ∙ clinical trials ∙ chemotherapy ∙ radiation therapy ∙ surgical therapy ∙ clinical observations ∙ clinical guidelines ∙ genetic consultation ∙ ethical considerations
Cancer Biology:
Molecular biology ∙ cellular biology ∙ molecular genetics ∙ genomics ∙ immunology ∙ epigenetics ∙ metabolic studies ∙ proteomics ∙ cytopathology ∙ carcinogenesis ∙ drug discovery and delivery.
Cancer Prevention:
Behavioral science ∙ psychosocial studies ∙ screening ∙ nutrition ∙ epidemiology and prevention ∙ community outreach.
Bioinformatics:
Gene expressions profiles ∙ gene regulation networks ∙ genome bioinformatics ∙ pathwayanalysis ∙ prognostic biomarkers.
Cancer Medicine publishes original research articles, systematic reviews, meta-analyses, and research methods papers, along with invited editorials and commentaries. Original research papers must report well-conducted research with conclusions supported by the data presented in the paper.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


