{"title":"食管癌患者术前的舌根肌肉质量与食管切除术后的吞咽功能有关。","authors":"Sanshiro Kawata, Yoshihiro Hiramatsu, Junko Honke, Tomohiro Murakami, Eisuke Booka, Tomohiro Matsumoto, Yoshifumi Morita, Hirotoshi Kikuchi, Katsuya Yamauchi, Hiroya Takeuchi","doi":"10.1002/ags3.12839","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>Dysphagia often develops after esophagectomy. The geniohyoid muscle is involved in swallowing movements, but its significance in esophagectomy patients remains unclear. We investigated the relationship of preoperative geniohyoid muscle mass with post-esophagectomy swallowing function.</p>\n </section>\n \n <section>\n \n <h3> Method<b>s</b></h3>\n \n <p>We retrospectively analyzed 114 patients who underwent esophagectomy and gastric conduit reconstruction for esophageal malignancy. We evaluated preoperative geniohyoid muscle sagittal cross-sectional areas (cm<sup>2</sup>) using computed tomography. Median values for each sex were considered as cutoff values. Dysphagia severity was assessed using the Penetration–Aspiration Scale (PAS) during video-fluoroscopic swallowing studies performed 7–10 days postoperatively.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>The cross-sectional area was significantly larger in males than in females (3.2 ± 0.7 vs. 2.4 ± 0.5, <i>p</i> < 0.01: median in males: 3.2 cm<sup>2</sup>, and in females: 2.3 cm<sup>2</sup>). These values were used to define high and low cross-sectional area groups. The cross-sectional area correlated positively with grip strength (correlation coefficient (CC) = 0.530) and skeletal muscle index (CC = 0.541). Transthyretin levels (22.4 ± 6.8 vs. 25.4 ± 5.5, <i>p</i> = 0.03) and cross-sectional area (2.6 ± 0.7 vs. 3.2 ± 0.8, <i>p</i> < 0.01) were significantly lower in patients with (PAS score ≥6; 20%) than in those without aspiration during fluoroscopic swallowing studies. Recurrent laryngeal nerve palsy was significantly more frequent in those with than in those without aspiration during fluoroscopic studies (22% vs. 5%, <i>p</i> = 0.03). In the multivariate analysis, low cross-sectional area and recurrent laryngeal nerve palsy were both independent risk factors for aspiration during swallowing studies (odds ratio = 3.6, <i>p</i> = 0.03 and odds ratio = 6.6, <i>p</i> = 0.02, respectively).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Preoperative geniohyoid muscle mass, evaluated using neck computed tomography, can predict dysphagia after esophagectomy.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 6","pages":"1026-1035"},"PeriodicalIF":2.9000,"publicationDate":"2024-06-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533026/pdf/","citationCount":"0","resultStr":"{\"title\":\"Preoperative geniohyoid muscle mass in esophageal cancer patients is associated with swallowing function after esophagectomy\",\"authors\":\"Sanshiro Kawata, Yoshihiro Hiramatsu, Junko Honke, Tomohiro Murakami, Eisuke Booka, Tomohiro Matsumoto, Yoshifumi Morita, Hirotoshi Kikuchi, Katsuya Yamauchi, Hiroya Takeuchi\",\"doi\":\"10.1002/ags3.12839\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>Dysphagia often develops after esophagectomy. The geniohyoid muscle is involved in swallowing movements, but its significance in esophagectomy patients remains unclear. We investigated the relationship of preoperative geniohyoid muscle mass with post-esophagectomy swallowing function.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Method<b>s</b></h3>\\n \\n <p>We retrospectively analyzed 114 patients who underwent esophagectomy and gastric conduit reconstruction for esophageal malignancy. We evaluated preoperative geniohyoid muscle sagittal cross-sectional areas (cm<sup>2</sup>) using computed tomography. Median values for each sex were considered as cutoff values. Dysphagia severity was assessed using the Penetration–Aspiration Scale (PAS) during video-fluoroscopic swallowing studies performed 7–10 days postoperatively.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>The cross-sectional area was significantly larger in males than in females (3.2 ± 0.7 vs. 2.4 ± 0.5, <i>p</i> < 0.01: median in males: 3.2 cm<sup>2</sup>, and in females: 2.3 cm<sup>2</sup>). These values were used to define high and low cross-sectional area groups. The cross-sectional area correlated positively with grip strength (correlation coefficient (CC) = 0.530) and skeletal muscle index (CC = 0.541). Transthyretin levels (22.4 ± 6.8 vs. 25.4 ± 5.5, <i>p</i> = 0.03) and cross-sectional area (2.6 ± 0.7 vs. 3.2 ± 0.8, <i>p</i> < 0.01) were significantly lower in patients with (PAS score ≥6; 20%) than in those without aspiration during fluoroscopic swallowing studies. Recurrent laryngeal nerve palsy was significantly more frequent in those with than in those without aspiration during fluoroscopic studies (22% vs. 5%, <i>p</i> = 0.03). In the multivariate analysis, low cross-sectional area and recurrent laryngeal nerve palsy were both independent risk factors for aspiration during swallowing studies (odds ratio = 3.6, <i>p</i> = 0.03 and odds ratio = 6.6, <i>p</i> = 0.02, respectively).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Preoperative geniohyoid muscle mass, evaluated using neck computed tomography, can predict dysphagia after esophagectomy.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 6\",\"pages\":\"1026-1035\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-06-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533026/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12839\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12839","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Preoperative geniohyoid muscle mass in esophageal cancer patients is associated with swallowing function after esophagectomy
Aim
Dysphagia often develops after esophagectomy. The geniohyoid muscle is involved in swallowing movements, but its significance in esophagectomy patients remains unclear. We investigated the relationship of preoperative geniohyoid muscle mass with post-esophagectomy swallowing function.
Methods
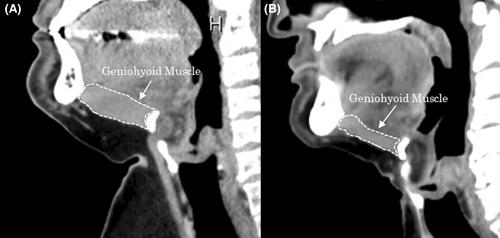
We retrospectively analyzed 114 patients who underwent esophagectomy and gastric conduit reconstruction for esophageal malignancy. We evaluated preoperative geniohyoid muscle sagittal cross-sectional areas (cm2) using computed tomography. Median values for each sex were considered as cutoff values. Dysphagia severity was assessed using the Penetration–Aspiration Scale (PAS) during video-fluoroscopic swallowing studies performed 7–10 days postoperatively.
Results
The cross-sectional area was significantly larger in males than in females (3.2 ± 0.7 vs. 2.4 ± 0.5, p < 0.01: median in males: 3.2 cm2, and in females: 2.3 cm2). These values were used to define high and low cross-sectional area groups. The cross-sectional area correlated positively with grip strength (correlation coefficient (CC) = 0.530) and skeletal muscle index (CC = 0.541). Transthyretin levels (22.4 ± 6.8 vs. 25.4 ± 5.5, p = 0.03) and cross-sectional area (2.6 ± 0.7 vs. 3.2 ± 0.8, p < 0.01) were significantly lower in patients with (PAS score ≥6; 20%) than in those without aspiration during fluoroscopic swallowing studies. Recurrent laryngeal nerve palsy was significantly more frequent in those with than in those without aspiration during fluoroscopic studies (22% vs. 5%, p = 0.03). In the multivariate analysis, low cross-sectional area and recurrent laryngeal nerve palsy were both independent risk factors for aspiration during swallowing studies (odds ratio = 3.6, p = 0.03 and odds ratio = 6.6, p = 0.02, respectively).
Conclusion
Preoperative geniohyoid muscle mass, evaluated using neck computed tomography, can predict dysphagia after esophagectomy.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


