Yoshinori Kagawa, Koji Ando, Mamoru Uemura, Jun Watanabe, Koji Oba, Yasunori Emi, Nobuhisa Matsuhashi, Naoki Izawa, Osamu Muto, Tatsuya Kinjo, Ichiro Takemasa, Eiji Oki
{"title":"日本对局部晚期直肠癌采用长程化放疗后巩固化疗作为新辅助治疗的 II 期研究:ENSEMBLE-2。","authors":"Yoshinori Kagawa, Koji Ando, Mamoru Uemura, Jun Watanabe, Koji Oba, Yasunori Emi, Nobuhisa Matsuhashi, Naoki Izawa, Osamu Muto, Tatsuya Kinjo, Ichiro Takemasa, Eiji Oki","doi":"10.1002/ags3.12848","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>To evaluate the feasibility and safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>This prospective, multicenter, single-arm, phase II trial was conducted at 10 centers. The eligibility criteria included age ≥20 y, locally advanced rectal cancer within 12 cm of the anal verge, and cT3-4N0M or TanyN+M0 at diagnosis, enabling curative resection. The protocol treatment was capecitabine (1650 mg/m<sup>2</sup>/day)-based long-course chemoradiotherapy (50.4 Gy/28 fractions) and consolidation chemotherapy (CAPOX, four courses) followed by total mesorectal excision. Nonoperative management was allowed if a clinical complete response was achieved. The primary endpoint was the pathologic complete response rate.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Among 28 enrolled patients (19 men, 9 women; median age, 69.5 [41–79] y), the long-course chemoradiotherapy and consolidation chemotherapy completion rates were 100% and 96.4%, respectively. The clinical responses included clinical complete response, (35.7%, 10/28), near-complete response (28.6%, 8/28), and incomplete response (32.1%, 9/28). Total mesorectal excision and nonoperative management were performed in 21 and six patients, respectively. The final analysis included 21 patients. Five patients (23.8% [90% confidence interval 11.8%–41.8%]) achieved pathologic complete response, while 10 of 28 patients (35.7%) achieved a pathological complete response or a sustained clinical complete response. No treatment-related deaths occurred. Grade ≥3 adverse events included diarrhea (7.1%) and leukopenia (7.1%).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>ENSEMBLE-2 demonstrated comparable pathologic complete response rates and well-tolerated safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.</p>\n </section>\n </div>","PeriodicalId":8030,"journal":{"name":"Annals of Gastroenterological Surgery","volume":"8 6","pages":"1067-1075"},"PeriodicalIF":3.3000,"publicationDate":"2024-08-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533031/pdf/","citationCount":"0","resultStr":"{\"title\":\"Phase II study of long-course chemoradiotherapy followed by consolidation chemotherapy as total neoadjuvant therapy in locally advanced rectal cancer in Japan: ENSEMBLE-2\",\"authors\":\"Yoshinori Kagawa, Koji Ando, Mamoru Uemura, Jun Watanabe, Koji Oba, Yasunori Emi, Nobuhisa Matsuhashi, Naoki Izawa, Osamu Muto, Tatsuya Kinjo, Ichiro Takemasa, Eiji Oki\",\"doi\":\"10.1002/ags3.12848\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>To evaluate the feasibility and safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>This prospective, multicenter, single-arm, phase II trial was conducted at 10 centers. The eligibility criteria included age ≥20 y, locally advanced rectal cancer within 12 cm of the anal verge, and cT3-4N0M or TanyN+M0 at diagnosis, enabling curative resection. The protocol treatment was capecitabine (1650 mg/m<sup>2</sup>/day)-based long-course chemoradiotherapy (50.4 Gy/28 fractions) and consolidation chemotherapy (CAPOX, four courses) followed by total mesorectal excision. Nonoperative management was allowed if a clinical complete response was achieved. The primary endpoint was the pathologic complete response rate.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Among 28 enrolled patients (19 men, 9 women; median age, 69.5 [41–79] y), the long-course chemoradiotherapy and consolidation chemotherapy completion rates were 100% and 96.4%, respectively. The clinical responses included clinical complete response, (35.7%, 10/28), near-complete response (28.6%, 8/28), and incomplete response (32.1%, 9/28). Total mesorectal excision and nonoperative management were performed in 21 and six patients, respectively. The final analysis included 21 patients. Five patients (23.8% [90% confidence interval 11.8%–41.8%]) achieved pathologic complete response, while 10 of 28 patients (35.7%) achieved a pathological complete response or a sustained clinical complete response. No treatment-related deaths occurred. Grade ≥3 adverse events included diarrhea (7.1%) and leukopenia (7.1%).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>ENSEMBLE-2 demonstrated comparable pathologic complete response rates and well-tolerated safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.</p>\\n </section>\\n </div>\",\"PeriodicalId\":8030,\"journal\":{\"name\":\"Annals of Gastroenterological Surgery\",\"volume\":\"8 6\",\"pages\":\"1067-1075\"},\"PeriodicalIF\":3.3000,\"publicationDate\":\"2024-08-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11533031/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Annals of Gastroenterological Surgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12848\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Annals of Gastroenterological Surgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ags3.12848","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Phase II study of long-course chemoradiotherapy followed by consolidation chemotherapy as total neoadjuvant therapy in locally advanced rectal cancer in Japan: ENSEMBLE-2
Aim
To evaluate the feasibility and safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.
Methods
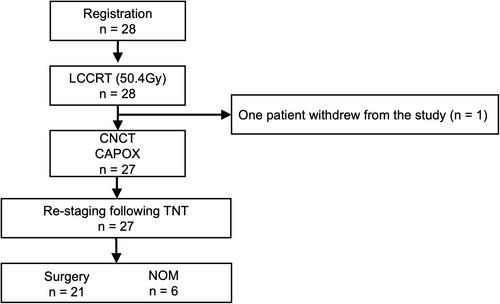
This prospective, multicenter, single-arm, phase II trial was conducted at 10 centers. The eligibility criteria included age ≥20 y, locally advanced rectal cancer within 12 cm of the anal verge, and cT3-4N0M or TanyN+M0 at diagnosis, enabling curative resection. The protocol treatment was capecitabine (1650 mg/m2/day)-based long-course chemoradiotherapy (50.4 Gy/28 fractions) and consolidation chemotherapy (CAPOX, four courses) followed by total mesorectal excision. Nonoperative management was allowed if a clinical complete response was achieved. The primary endpoint was the pathologic complete response rate.
Results
Among 28 enrolled patients (19 men, 9 women; median age, 69.5 [41–79] y), the long-course chemoradiotherapy and consolidation chemotherapy completion rates were 100% and 96.4%, respectively. The clinical responses included clinical complete response, (35.7%, 10/28), near-complete response (28.6%, 8/28), and incomplete response (32.1%, 9/28). Total mesorectal excision and nonoperative management were performed in 21 and six patients, respectively. The final analysis included 21 patients. Five patients (23.8% [90% confidence interval 11.8%–41.8%]) achieved pathologic complete response, while 10 of 28 patients (35.7%) achieved a pathological complete response or a sustained clinical complete response. No treatment-related deaths occurred. Grade ≥3 adverse events included diarrhea (7.1%) and leukopenia (7.1%).
Conclusion
ENSEMBLE-2 demonstrated comparable pathologic complete response rates and well-tolerated safety of total neoadjuvant therapy with long-course chemoradiotherapy followed by consolidation chemotherapy in Japanese patients with locally advanced rectal cancer.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


