Tauben Averbuch, Shun Fu Lee, Brandon Zagorski, Ambarish Pandey, Mark C. Petrie, Tor Biering-Sorensen, Feng Xie, Harriette G.C. Van Spall
{"title":"男性和女性心力衰竭住院患者的长期临床疗效和医疗资源使用情况。","authors":"Tauben Averbuch, Shun Fu Lee, Brandon Zagorski, Ambarish Pandey, Mark C. Petrie, Tor Biering-Sorensen, Feng Xie, Harriette G.C. Van Spall","doi":"10.1002/ejhf.3499","DOIUrl":null,"url":null,"abstract":"<div>\n \n <section>\n \n <h3> Aims</h3>\n \n <p>Heart failure (HF) is a leading cause of hospitalization, and sex differences in care have been described. We assessed sex-specific clinical outcomes and healthcare resource utilization following hospitalization for HF.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>This was an exploratory analysis of patients hospitalized for HF across 10 Canadian hospitals in the Patient-Centered Care Transitions in HF (PACT-HF) cluster-randomized trial. The primary outcome was all-cause mortality. Secondary outcomes included all-cause readmissions, HF readmissions, emergency department (ED) visits, and healthcare resource utilization. Outcomes were obtained via linkages with administrative datasets. Among 4441 patients discharged alive, 50.7% were female. By 5 years, 63.6% and 65.5% of male and female patients, respectively, had died (<i>p</i> = 0.19); 85.4% and 84.4%, respectively, were readmitted (<i>p</i> = 0.35); and 72.2% and 70.9%, respectively, received ED care without hospitalization (<i>p</i> = 0.34). There were no sex differences in mean [SD] number of all-cause readmissions (males, 2.8 [7.8] and females, 3.0 [8.4], <i>p</i> = 0.54), HF readmissions (males, 0.9 [3.6] and females, 0.9 [4.5], <i>p</i> = 0.80), or ED visits (males, 1.8 [11.3] and females, 1.5 [6.0], <i>p</i> = 0.24) per person. There were no sex differences in mean [SD] annual direct healthcare cost per patient (males, $80 334 [116 762] versus females, $81 010 [112 625], <i>p</i> = 0.90), but males received more specialist, multidisciplinary HF clinic, haemodialysis, and day surgical care, and females received more home visits, continuing/convalescent care, and long-term care. Annualized clinical events were highest in first year following index discharge in both males and females.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Among people discharged alive after hospitalization for HF, there were no sex differences in total and annual deaths, readmissions, and ED visits, or in total direct healthcare costs. Despite similar risk profiles, males received relatively more specialist care and day surgical procedures, and females received more supportive care.</p>\n \n <p>Clinical Trial Registration: ClinicalTrials.gov NCT02112227.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"27 2","pages":"377-387"},"PeriodicalIF":16.9000,"publicationDate":"2024-11-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3499","citationCount":"0","resultStr":"{\"title\":\"Long-term clinical outcomes and healthcare resource utilization in male and female patients following hospitalization for heart failure\",\"authors\":\"Tauben Averbuch, Shun Fu Lee, Brandon Zagorski, Ambarish Pandey, Mark C. Petrie, Tor Biering-Sorensen, Feng Xie, Harriette G.C. Van Spall\",\"doi\":\"10.1002/ejhf.3499\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>Heart failure (HF) is a leading cause of hospitalization, and sex differences in care have been described. We assessed sex-specific clinical outcomes and healthcare resource utilization following hospitalization for HF.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>This was an exploratory analysis of patients hospitalized for HF across 10 Canadian hospitals in the Patient-Centered Care Transitions in HF (PACT-HF) cluster-randomized trial. The primary outcome was all-cause mortality. Secondary outcomes included all-cause readmissions, HF readmissions, emergency department (ED) visits, and healthcare resource utilization. Outcomes were obtained via linkages with administrative datasets. Among 4441 patients discharged alive, 50.7% were female. By 5 years, 63.6% and 65.5% of male and female patients, respectively, had died (<i>p</i> = 0.19); 85.4% and 84.4%, respectively, were readmitted (<i>p</i> = 0.35); and 72.2% and 70.9%, respectively, received ED care without hospitalization (<i>p</i> = 0.34). There were no sex differences in mean [SD] number of all-cause readmissions (males, 2.8 [7.8] and females, 3.0 [8.4], <i>p</i> = 0.54), HF readmissions (males, 0.9 [3.6] and females, 0.9 [4.5], <i>p</i> = 0.80), or ED visits (males, 1.8 [11.3] and females, 1.5 [6.0], <i>p</i> = 0.24) per person. There were no sex differences in mean [SD] annual direct healthcare cost per patient (males, $80 334 [116 762] versus females, $81 010 [112 625], <i>p</i> = 0.90), but males received more specialist, multidisciplinary HF clinic, haemodialysis, and day surgical care, and females received more home visits, continuing/convalescent care, and long-term care. Annualized clinical events were highest in first year following index discharge in both males and females.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Among people discharged alive after hospitalization for HF, there were no sex differences in total and annual deaths, readmissions, and ED visits, or in total direct healthcare costs. Despite similar risk profiles, males received relatively more specialist care and day surgical procedures, and females received more supportive care.</p>\\n \\n <p>Clinical Trial Registration: ClinicalTrials.gov NCT02112227.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"27 2\",\"pages\":\"377-387\"},\"PeriodicalIF\":16.9000,\"publicationDate\":\"2024-11-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/ejhf.3499\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3499\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3499","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Long-term clinical outcomes and healthcare resource utilization in male and female patients following hospitalization for heart failure
Aims
Heart failure (HF) is a leading cause of hospitalization, and sex differences in care have been described. We assessed sex-specific clinical outcomes and healthcare resource utilization following hospitalization for HF.
Methods and results
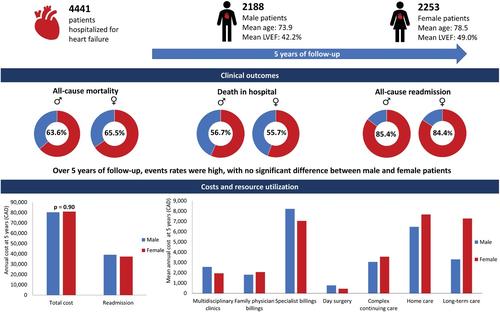
This was an exploratory analysis of patients hospitalized for HF across 10 Canadian hospitals in the Patient-Centered Care Transitions in HF (PACT-HF) cluster-randomized trial. The primary outcome was all-cause mortality. Secondary outcomes included all-cause readmissions, HF readmissions, emergency department (ED) visits, and healthcare resource utilization. Outcomes were obtained via linkages with administrative datasets. Among 4441 patients discharged alive, 50.7% were female. By 5 years, 63.6% and 65.5% of male and female patients, respectively, had died (p = 0.19); 85.4% and 84.4%, respectively, were readmitted (p = 0.35); and 72.2% and 70.9%, respectively, received ED care without hospitalization (p = 0.34). There were no sex differences in mean [SD] number of all-cause readmissions (males, 2.8 [7.8] and females, 3.0 [8.4], p = 0.54), HF readmissions (males, 0.9 [3.6] and females, 0.9 [4.5], p = 0.80), or ED visits (males, 1.8 [11.3] and females, 1.5 [6.0], p = 0.24) per person. There were no sex differences in mean [SD] annual direct healthcare cost per patient (males, $80 334 [116 762] versus females, $81 010 [112 625], p = 0.90), but males received more specialist, multidisciplinary HF clinic, haemodialysis, and day surgical care, and females received more home visits, continuing/convalescent care, and long-term care. Annualized clinical events were highest in first year following index discharge in both males and females.
Conclusions
Among people discharged alive after hospitalization for HF, there were no sex differences in total and annual deaths, readmissions, and ED visits, or in total direct healthcare costs. Despite similar risk profiles, males received relatively more specialist care and day surgical procedures, and females received more supportive care.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


