Lauryn J Boggs, Ishan Patel, Melina Holyszko, Bryan E Little, Hussein F Darwiche, Rahul Vaidya
{"title":"使用底特律介入性疼痛评估量表评估全关节置换术中的疼痛管理--前瞻性队列研究。","authors":"Lauryn J Boggs, Ishan Patel, Melina Holyszko, Bryan E Little, Hussein F Darwiche, Rahul Vaidya","doi":"10.1186/s42836-024-00276-w","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Total joint arthroplasty (TJA) is an effective treatment for end-stage osteoarthritis, but postoperative pain has been poorly managed. The purpose of this study was to (1) assess how much narcotic medication was prescribed after TJA; (2) assess if patients were satisfied with their pain management; (3) compare these same data between total hip arthroplasty (THA)/total knee arthroplasty (TKA); (4) compare these same data between preoperative opioid users/opioid-naïve patients.</p><p><strong>Methods: </strong>An IRB-approved prospective study was conducted at a US academic joint replacement practice. Patients were evaluated by an independent observer at three weeks, three months, and six months postoperatively using the Detroit Interventional Pain Assessment (DIPA) scale. Patients verbally rated their pain with their current medication regimen as 0 (no pain), 1 (tolerable pain), or 2 (intolerable pain) on the DIPA scale. Narcotic usage was verified by the Michigan Automated Prescription System (MAPS). Patients were divided into THA, TKA, previously on opioids, and opioid-naïve groups. Provider efficiency scores reflected pain management satisfaction and were calculated as the percentage of patients reporting no pain or tolerable pain.</p><p><strong>Results: </strong>Out of 200 patients, the percentage of patients using narcotics and their daily usage (MMEs) significantly decreased from 75.5% (27.5 MMEs) at three weeks to 42.9% (5.3 MMEs) at six months (P < 0.001). In 80% of patients, narcotics taken at six months were prescribed by outside providers. Significantly fewer patients used narcotics at six months for THA (15.4%) compared to TKA (52.7%) (P < 0.021). There was a significant difference in daily narcotic usage between patients who took narcotics preoperatively (22.9 MMEs) and opioid-naïve ones (13.4 MMEs) (P < 0.001). Provider efficiency scores were best at three weeks (76.6%) and three months (70%) but declined at six months (57.2%).</p><p><strong>Conclusions: </strong>Narcotic tapering practices were observed as postoperative daily narcotic intake decreased across six months. However, outside providers prescribed 80% of narcotics at six months, necessitating a better-coordinated practice with surgeons. Patients taking preoperative narcotics experienced higher daily MME requirements than their opioid-naïve counterparts. In terms of the percentage of patients on narcotics, THA is a better procedure for tapering patients off narcotics by six months.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"6 1","pages":"55"},"PeriodicalIF":4.3000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11529018/pdf/","citationCount":"0","resultStr":"{\"title\":\"Assessing pain management in total joint arthroplasty using the Detroit interventional pain assessment scale-A prospective cohort study.\",\"authors\":\"Lauryn J Boggs, Ishan Patel, Melina Holyszko, Bryan E Little, Hussein F Darwiche, Rahul Vaidya\",\"doi\":\"10.1186/s42836-024-00276-w\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Total joint arthroplasty (TJA) is an effective treatment for end-stage osteoarthritis, but postoperative pain has been poorly managed. The purpose of this study was to (1) assess how much narcotic medication was prescribed after TJA; (2) assess if patients were satisfied with their pain management; (3) compare these same data between total hip arthroplasty (THA)/total knee arthroplasty (TKA); (4) compare these same data between preoperative opioid users/opioid-naïve patients.</p><p><strong>Methods: </strong>An IRB-approved prospective study was conducted at a US academic joint replacement practice. Patients were evaluated by an independent observer at three weeks, three months, and six months postoperatively using the Detroit Interventional Pain Assessment (DIPA) scale. Patients verbally rated their pain with their current medication regimen as 0 (no pain), 1 (tolerable pain), or 2 (intolerable pain) on the DIPA scale. Narcotic usage was verified by the Michigan Automated Prescription System (MAPS). Patients were divided into THA, TKA, previously on opioids, and opioid-naïve groups. Provider efficiency scores reflected pain management satisfaction and were calculated as the percentage of patients reporting no pain or tolerable pain.</p><p><strong>Results: </strong>Out of 200 patients, the percentage of patients using narcotics and their daily usage (MMEs) significantly decreased from 75.5% (27.5 MMEs) at three weeks to 42.9% (5.3 MMEs) at six months (P < 0.001). In 80% of patients, narcotics taken at six months were prescribed by outside providers. Significantly fewer patients used narcotics at six months for THA (15.4%) compared to TKA (52.7%) (P < 0.021). There was a significant difference in daily narcotic usage between patients who took narcotics preoperatively (22.9 MMEs) and opioid-naïve ones (13.4 MMEs) (P < 0.001). Provider efficiency scores were best at three weeks (76.6%) and three months (70%) but declined at six months (57.2%).</p><p><strong>Conclusions: </strong>Narcotic tapering practices were observed as postoperative daily narcotic intake decreased across six months. However, outside providers prescribed 80% of narcotics at six months, necessitating a better-coordinated practice with surgeons. Patients taking preoperative narcotics experienced higher daily MME requirements than their opioid-naïve counterparts. In terms of the percentage of patients on narcotics, THA is a better procedure for tapering patients off narcotics by six months.</p>\",\"PeriodicalId\":52831,\"journal\":{\"name\":\"Arthroplasty\",\"volume\":\"6 1\",\"pages\":\"55\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11529018/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthroplasty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s42836-024-00276-w\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-024-00276-w","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Assessing pain management in total joint arthroplasty using the Detroit interventional pain assessment scale-A prospective cohort study.
Background: Total joint arthroplasty (TJA) is an effective treatment for end-stage osteoarthritis, but postoperative pain has been poorly managed. The purpose of this study was to (1) assess how much narcotic medication was prescribed after TJA; (2) assess if patients were satisfied with their pain management; (3) compare these same data between total hip arthroplasty (THA)/total knee arthroplasty (TKA); (4) compare these same data between preoperative opioid users/opioid-naïve patients.
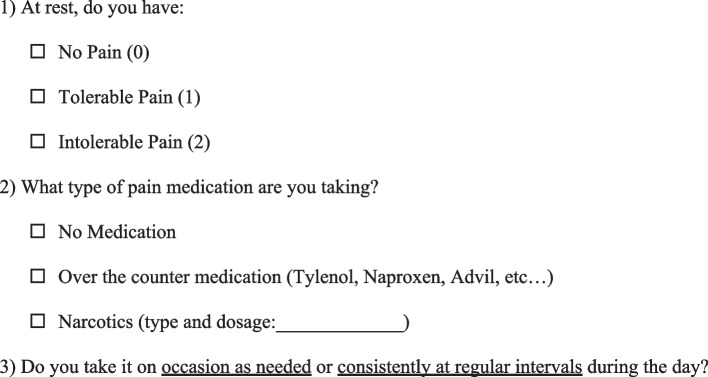
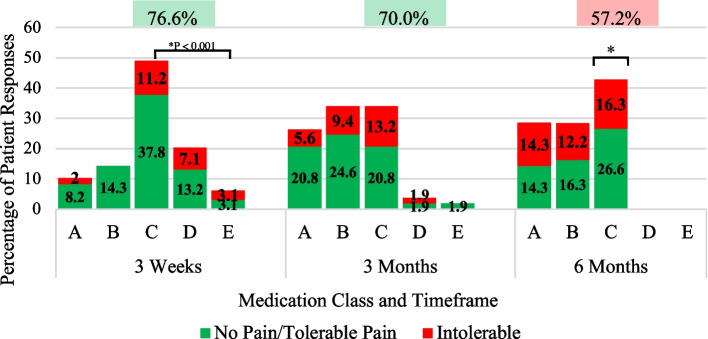
Methods: An IRB-approved prospective study was conducted at a US academic joint replacement practice. Patients were evaluated by an independent observer at three weeks, three months, and six months postoperatively using the Detroit Interventional Pain Assessment (DIPA) scale. Patients verbally rated their pain with their current medication regimen as 0 (no pain), 1 (tolerable pain), or 2 (intolerable pain) on the DIPA scale. Narcotic usage was verified by the Michigan Automated Prescription System (MAPS). Patients were divided into THA, TKA, previously on opioids, and opioid-naïve groups. Provider efficiency scores reflected pain management satisfaction and were calculated as the percentage of patients reporting no pain or tolerable pain.
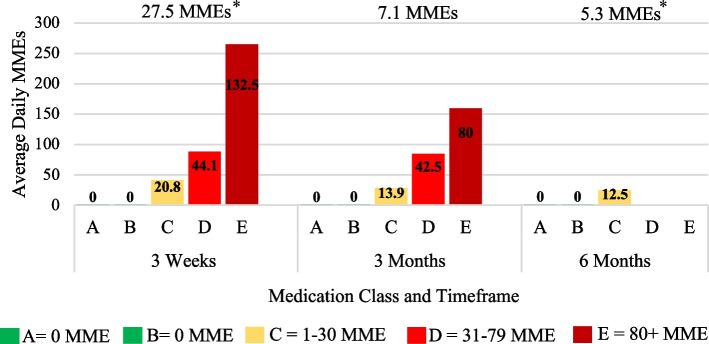
Results: Out of 200 patients, the percentage of patients using narcotics and their daily usage (MMEs) significantly decreased from 75.5% (27.5 MMEs) at three weeks to 42.9% (5.3 MMEs) at six months (P < 0.001). In 80% of patients, narcotics taken at six months were prescribed by outside providers. Significantly fewer patients used narcotics at six months for THA (15.4%) compared to TKA (52.7%) (P < 0.021). There was a significant difference in daily narcotic usage between patients who took narcotics preoperatively (22.9 MMEs) and opioid-naïve ones (13.4 MMEs) (P < 0.001). Provider efficiency scores were best at three weeks (76.6%) and three months (70%) but declined at six months (57.2%).
Conclusions: Narcotic tapering practices were observed as postoperative daily narcotic intake decreased across six months. However, outside providers prescribed 80% of narcotics at six months, necessitating a better-coordinated practice with surgeons. Patients taking preoperative narcotics experienced higher daily MME requirements than their opioid-naïve counterparts. In terms of the percentage of patients on narcotics, THA is a better procedure for tapering patients off narcotics by six months.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


