{"title":"糖尿病患者因细金丝桃而自发形成大面积皮下脓肿:病例报告。","authors":"Toshiyuki Sato, Mayuka Tomita, Atsuhiro Kohno, Satomi Chujo, Yuma Waki, Yoshimasa Nobeyama, Masaaki Kawase, Akihiko Asahina","doi":"10.1159/000540636","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong><i>Finegoldia magna</i> is a member of the Gram-positive anaerobic cocci group and constitutes the flora of the skin and other parts of the body. It sometimes colonizes diabetic foot and rarely infects skin or soft tissue of non-immunocompromised patients.</p><p><strong>Case presentation: </strong>Here, we report the case of a severe subcutaneous abscess on the back caused by <i>F</i>. <i>magna</i> involving an immunocompromised patient with poorly controlled diabetes. A 48-year-old woman with diabetes mellitus and anemia associated with uterine fibroids was referred to us with a 1-month history of a skin manifestation on her back, with a body temperature of 35.9°C and blood pressure of 115/73 mm Hg. The manifestation involved a subcutaneous mass of 36 × 45 cm with a foul odor, partly covered with necrotic tissue, which had the appearance of a tortoiseshell-like pattern. Blood examination revealed C-reactive protein of 21.4 mg/dL and hemoglobin A1c of 9.1%. Contrast-enhanced computed tomography showed a subcutaneous abscess with internal emphysema. Emergency debridement was performed, resulting in drainage of foul-smelling gray-green pus. <i>F</i>. <i>magna</i> was detected in the pus and skin tissue.</p><p><strong>Conclusion: </strong>Skin and soft tissue infectious disease caused by <i>F</i>. <i>magna</i> is extremely rare, but the disease tends to become severe once developing in an immunocompromised patient, such as a patient with poorly controlled diabetes. Therefore, physicians should consider <i>F</i>. <i>magna</i> as a causative agent when poorly controlled diabetic patients suffer from severe infectious cutaneous manifestations.</p>","PeriodicalId":9619,"journal":{"name":"Case Reports in Dermatology","volume":"16 1","pages":"202-209"},"PeriodicalIF":0.8000,"publicationDate":"2024-08-23","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11521465/pdf/","citationCount":"0","resultStr":"{\"title\":\"Large Spontaneous Subcutaneous Abscess Formation due to <i>Finegoldia magna</i> in a Diabetic Patient: A Case Report.\",\"authors\":\"Toshiyuki Sato, Mayuka Tomita, Atsuhiro Kohno, Satomi Chujo, Yuma Waki, Yoshimasa Nobeyama, Masaaki Kawase, Akihiko Asahina\",\"doi\":\"10.1159/000540636\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong><i>Finegoldia magna</i> is a member of the Gram-positive anaerobic cocci group and constitutes the flora of the skin and other parts of the body. It sometimes colonizes diabetic foot and rarely infects skin or soft tissue of non-immunocompromised patients.</p><p><strong>Case presentation: </strong>Here, we report the case of a severe subcutaneous abscess on the back caused by <i>F</i>. <i>magna</i> involving an immunocompromised patient with poorly controlled diabetes. A 48-year-old woman with diabetes mellitus and anemia associated with uterine fibroids was referred to us with a 1-month history of a skin manifestation on her back, with a body temperature of 35.9°C and blood pressure of 115/73 mm Hg. The manifestation involved a subcutaneous mass of 36 × 45 cm with a foul odor, partly covered with necrotic tissue, which had the appearance of a tortoiseshell-like pattern. Blood examination revealed C-reactive protein of 21.4 mg/dL and hemoglobin A1c of 9.1%. Contrast-enhanced computed tomography showed a subcutaneous abscess with internal emphysema. Emergency debridement was performed, resulting in drainage of foul-smelling gray-green pus. <i>F</i>. <i>magna</i> was detected in the pus and skin tissue.</p><p><strong>Conclusion: </strong>Skin and soft tissue infectious disease caused by <i>F</i>. <i>magna</i> is extremely rare, but the disease tends to become severe once developing in an immunocompromised patient, such as a patient with poorly controlled diabetes. Therefore, physicians should consider <i>F</i>. <i>magna</i> as a causative agent when poorly controlled diabetic patients suffer from severe infectious cutaneous manifestations.</p>\",\"PeriodicalId\":9619,\"journal\":{\"name\":\"Case Reports in Dermatology\",\"volume\":\"16 1\",\"pages\":\"202-209\"},\"PeriodicalIF\":0.8000,\"publicationDate\":\"2024-08-23\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11521465/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Case Reports in Dermatology\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1159/000540636\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q4\",\"JCRName\":\"DERMATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Case Reports in Dermatology","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1159/000540636","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q4","JCRName":"DERMATOLOGY","Score":null,"Total":0}
Large Spontaneous Subcutaneous Abscess Formation due to Finegoldia magna in a Diabetic Patient: A Case Report.
Introduction: Finegoldia magna is a member of the Gram-positive anaerobic cocci group and constitutes the flora of the skin and other parts of the body. It sometimes colonizes diabetic foot and rarely infects skin or soft tissue of non-immunocompromised patients.
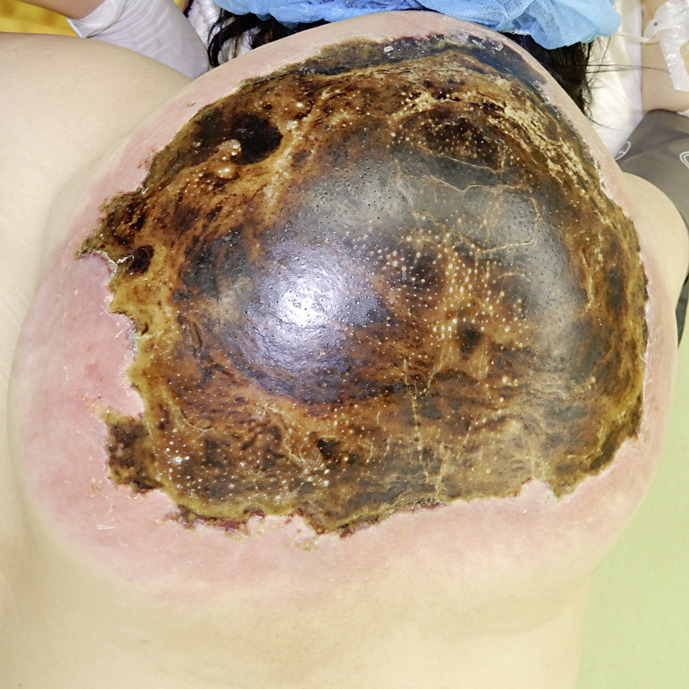
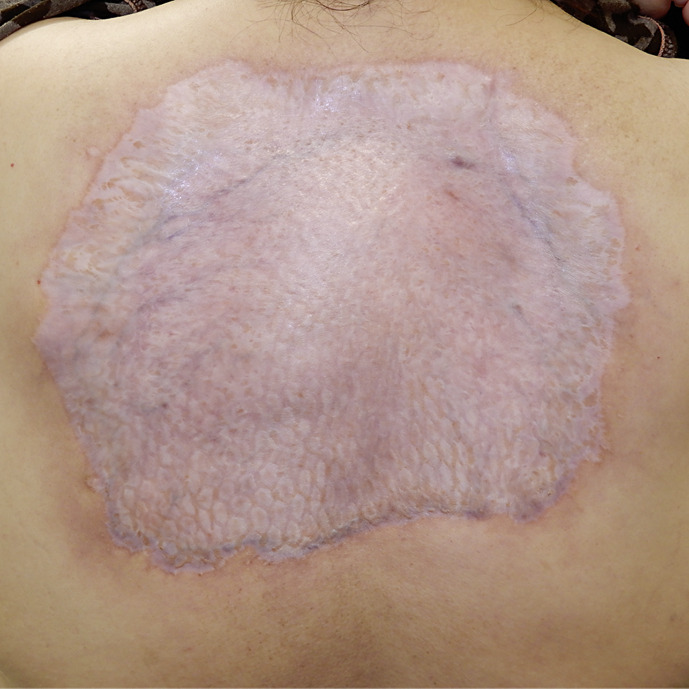
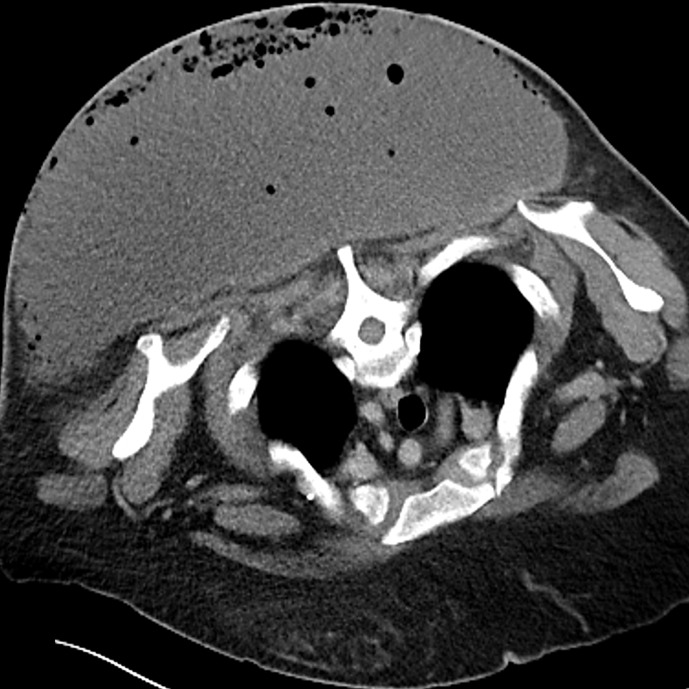
Case presentation: Here, we report the case of a severe subcutaneous abscess on the back caused by F. magna involving an immunocompromised patient with poorly controlled diabetes. A 48-year-old woman with diabetes mellitus and anemia associated with uterine fibroids was referred to us with a 1-month history of a skin manifestation on her back, with a body temperature of 35.9°C and blood pressure of 115/73 mm Hg. The manifestation involved a subcutaneous mass of 36 × 45 cm with a foul odor, partly covered with necrotic tissue, which had the appearance of a tortoiseshell-like pattern. Blood examination revealed C-reactive protein of 21.4 mg/dL and hemoglobin A1c of 9.1%. Contrast-enhanced computed tomography showed a subcutaneous abscess with internal emphysema. Emergency debridement was performed, resulting in drainage of foul-smelling gray-green pus. F. magna was detected in the pus and skin tissue.
Conclusion: Skin and soft tissue infectious disease caused by F. magna is extremely rare, but the disease tends to become severe once developing in an immunocompromised patient, such as a patient with poorly controlled diabetes. Therefore, physicians should consider F. magna as a causative agent when poorly controlled diabetic patients suffer from severe infectious cutaneous manifestations.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


