{"title":"外伤性脾破裂揭示了腮腺炎与潜在的 B 细胞淋巴样增生:诊断难题。","authors":"Inderjeet Singh, Hariharasudhan Balaji, Nithin Jyothy","doi":"10.7759/cureus.72671","DOIUrl":null,"url":null,"abstract":"<p><p>Atraumatic splenic rupture (ASR) is an unfamiliar entity that is potentially life-threatening if there is a delay in the diagnosis. Due to its rarity and its non-specific presentation, it can be a challenge to diagnose early. In this report, we present a case of a 42-year-old male patient who presented to the emergency department with nonspecific abdominal pain and had no past medical history. The patient presented abdominal pain associated with nausea, vomiting, and sweating. On examination, the patient was found to be tachycardic and mildly hypotensive, with mild left upper quadrant tenderness, and a lactate of 4 mmol/L on venous blood gas analysis. He was urgently transferred to the resuscitation area, where resuscitation commenced. Further investigations revealed significant anemia. The contrast-enhanced CT of the abdomen performed revealed a 13-cm splenic hemostasis suggestive of non-traumatic splenic rupture. The patient lacked any history of blunt trauma or family history that could account for the splenic rupture. The patient was taken to the theatre by the surgical team as he remained unstable. He received four units of blood in the theatre and underwent splenectomy due to the spleen being unsalvageable. Post-operatively, the patient was admitted to the high-dependency unit (HDU) for close monitoring. Histological examination of the splenic tissue revealed B-cell lymphoid hyperplasia and negative PCR for clonality. The patient was found to be IgG-positive for mumps and was not vaccinated for MMR. Surgeons believe it is the main cause of ASR, given that little literature available establishes the same. The case highlights the importance of consideration of ASR in patients presenting with unexplained abdominal pain and hemodynamic instability, even without evidence of trauma. Early imaging and operative intervention are lifesaving. The histologic findings indicate that there may be an associated hemopoietic disorder, and this case highlights the need for clinicians to consider splenic involvement in patients with mumps who present with abdominal pain or signs of hemodynamic instability.</p>","PeriodicalId":93960,"journal":{"name":"Cureus","volume":"16 10","pages":"e72671"},"PeriodicalIF":1.3000,"publicationDate":"2024-10-29","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11523189/pdf/","citationCount":"0","resultStr":"{\"title\":\"Atraumatic Splenic Rupture Unveiling Mumps With an Underlying B-cell Lymphoid Hyperplasia: A Diagnostic Conundrum.\",\"authors\":\"Inderjeet Singh, Hariharasudhan Balaji, Nithin Jyothy\",\"doi\":\"10.7759/cureus.72671\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Atraumatic splenic rupture (ASR) is an unfamiliar entity that is potentially life-threatening if there is a delay in the diagnosis. Due to its rarity and its non-specific presentation, it can be a challenge to diagnose early. In this report, we present a case of a 42-year-old male patient who presented to the emergency department with nonspecific abdominal pain and had no past medical history. The patient presented abdominal pain associated with nausea, vomiting, and sweating. On examination, the patient was found to be tachycardic and mildly hypotensive, with mild left upper quadrant tenderness, and a lactate of 4 mmol/L on venous blood gas analysis. He was urgently transferred to the resuscitation area, where resuscitation commenced. Further investigations revealed significant anemia. The contrast-enhanced CT of the abdomen performed revealed a 13-cm splenic hemostasis suggestive of non-traumatic splenic rupture. The patient lacked any history of blunt trauma or family history that could account for the splenic rupture. The patient was taken to the theatre by the surgical team as he remained unstable. He received four units of blood in the theatre and underwent splenectomy due to the spleen being unsalvageable. Post-operatively, the patient was admitted to the high-dependency unit (HDU) for close monitoring. Histological examination of the splenic tissue revealed B-cell lymphoid hyperplasia and negative PCR for clonality. The patient was found to be IgG-positive for mumps and was not vaccinated for MMR. Surgeons believe it is the main cause of ASR, given that little literature available establishes the same. The case highlights the importance of consideration of ASR in patients presenting with unexplained abdominal pain and hemodynamic instability, even without evidence of trauma. Early imaging and operative intervention are lifesaving. The histologic findings indicate that there may be an associated hemopoietic disorder, and this case highlights the need for clinicians to consider splenic involvement in patients with mumps who present with abdominal pain or signs of hemodynamic instability.</p>\",\"PeriodicalId\":93960,\"journal\":{\"name\":\"Cureus\",\"volume\":\"16 10\",\"pages\":\"e72671\"},\"PeriodicalIF\":1.3000,\"publicationDate\":\"2024-10-29\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11523189/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Cureus\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.7759/cureus.72671\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Cureus","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.7759/cureus.72671","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
引用次数: 0
摘要
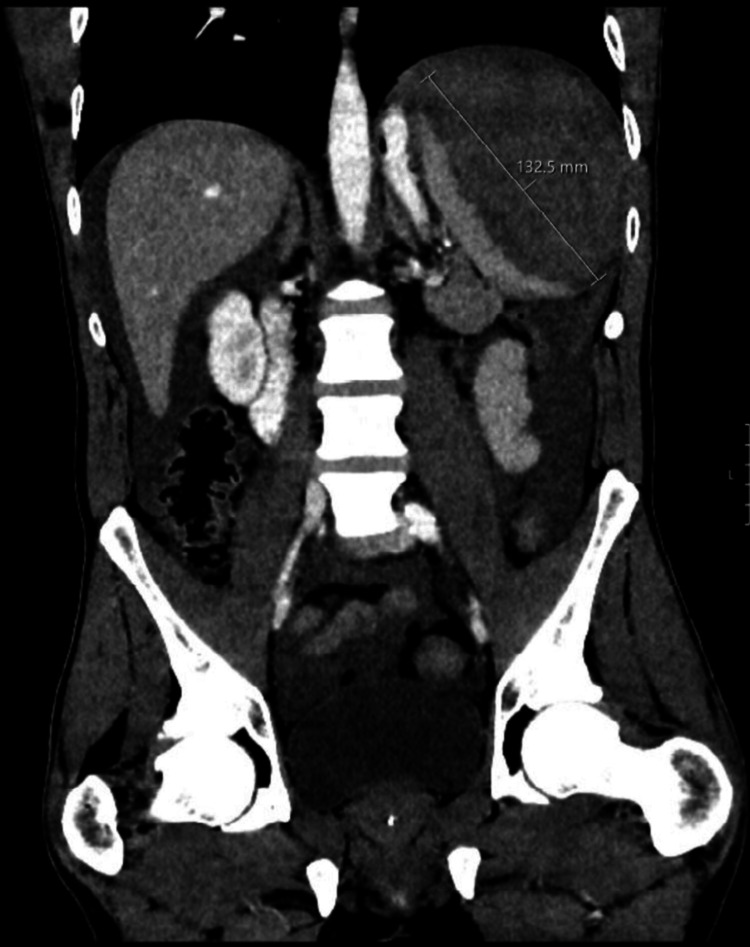
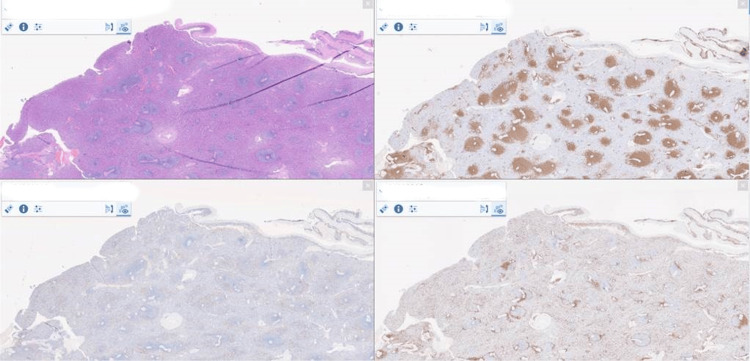
创伤性脾破裂(ASR)是一种陌生的疾病,如果诊断不及时,可能会危及生命。由于其罕见性和非特异性表现,早期诊断是一项挑战。在本报告中,我们介绍了一例因非特异性腹痛而到急诊科就诊的 42 岁男性患者,该患者无既往病史。患者表现为腹痛,伴有恶心、呕吐和出汗。检查发现,患者心动过速,轻度低血压,左上腹轻度压痛,静脉血气分析乳酸为4毫摩尔/升。他被紧急转移到抢救区,并开始进行抢救。进一步检查发现他有严重贫血。腹部对比增强 CT 显示有一个 13 厘米长的脾脏止血点,提示为非创伤性脾破裂。患者没有任何钝性外伤史或家族史,因此无法解释脾破裂的原因。由于病情仍不稳定,手术团队将患者送往手术室。他在手术室接受了四个单位的输血,并因脾脏无法修复而接受了脾脏切除术。术后,患者被送入重症监护室(HDU)接受密切监护。脾脏组织的组织学检查显示 B 细胞淋巴细胞增生,PCR 检测结果为阴性。患者腮腺炎 IgG 阳性,且未接种麻腮风疫苗。外科医生认为这是 ASR 的主要病因,因为几乎没有文献证实这一点。该病例强调,对于出现不明原因腹痛和血流动力学不稳定的患者,即使没有外伤证据,也必须考虑 ASR。早期成像和手术干预可以挽救生命。组织学检查结果表明可能存在相关的造血功能障碍,本病例强调临床医生需要考虑腹痛或血流动力学不稳定的腮腺炎患者的脾脏受累情况。
Atraumatic Splenic Rupture Unveiling Mumps With an Underlying B-cell Lymphoid Hyperplasia: A Diagnostic Conundrum.
Atraumatic splenic rupture (ASR) is an unfamiliar entity that is potentially life-threatening if there is a delay in the diagnosis. Due to its rarity and its non-specific presentation, it can be a challenge to diagnose early. In this report, we present a case of a 42-year-old male patient who presented to the emergency department with nonspecific abdominal pain and had no past medical history. The patient presented abdominal pain associated with nausea, vomiting, and sweating. On examination, the patient was found to be tachycardic and mildly hypotensive, with mild left upper quadrant tenderness, and a lactate of 4 mmol/L on venous blood gas analysis. He was urgently transferred to the resuscitation area, where resuscitation commenced. Further investigations revealed significant anemia. The contrast-enhanced CT of the abdomen performed revealed a 13-cm splenic hemostasis suggestive of non-traumatic splenic rupture. The patient lacked any history of blunt trauma or family history that could account for the splenic rupture. The patient was taken to the theatre by the surgical team as he remained unstable. He received four units of blood in the theatre and underwent splenectomy due to the spleen being unsalvageable. Post-operatively, the patient was admitted to the high-dependency unit (HDU) for close monitoring. Histological examination of the splenic tissue revealed B-cell lymphoid hyperplasia and negative PCR for clonality. The patient was found to be IgG-positive for mumps and was not vaccinated for MMR. Surgeons believe it is the main cause of ASR, given that little literature available establishes the same. The case highlights the importance of consideration of ASR in patients presenting with unexplained abdominal pain and hemodynamic instability, even without evidence of trauma. Early imaging and operative intervention are lifesaving. The histologic findings indicate that there may be an associated hemopoietic disorder, and this case highlights the need for clinicians to consider splenic involvement in patients with mumps who present with abdominal pain or signs of hemodynamic instability.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


