早期β-受体阻滞剂与艾司洛尔对严重创伤性脑损伤成人治疗强度水平的影响》(The Effect of Early Beta-Blockade with Esmolol on Therapy Intensity Level in Adults with Severe Traumatic Brainjury)。
Thomas Baumer, George Higginbotham, Kati Hayes, Matt Thomas
{"title":"早期β-受体阻滞剂与艾司洛尔对严重创伤性脑损伤成人治疗强度水平的影响》(The Effect of Early Beta-Blockade with Esmolol on Therapy Intensity Level in Adults with Severe Traumatic Brainjury)。","authors":"Thomas Baumer, George Higginbotham, Kati Hayes, Matt Thomas","doi":"10.1089/neur.2024.0055","DOIUrl":null,"url":null,"abstract":"<p><p>Following severe traumatic brain injury (TBI), elevated catecholamine levels are associated with worsened secondary brain injury and poorer clinical outcomes. The mechanisms are uncertain but may include cerebral ischemia and blood-brain barrier disruption, with consequent cerebral edema manifesting as intracranial hypertension. Early beta-blockade (EBB) may mitigate these detrimental hyperadrenergic effects. Therapy Intensity Level (TIL) is a validated score that quantifies intracranial pressure (ICP)-lowering interventions, with higher TIL being a surrogate for more severe intracranial hypertension. In this <i>post hoc</i> secondary analysis of a dose-finding study of EBB with esmolol in adults with TBI, we compared summary TIL (TIL24) and domain TIL between patients who received esmolol and those who did not. The primary outcome was TIL24 for each 24-h epoch of the esmolol intervention period of 96 h. Baseline characteristics were comparable in the esmolol (E) and non-esmolol (NE) groups. Mean TIL24 was similar in both groups up to 48 h but then diverged. The mean (standard deviation) TIL24 score between 48 and 72 h was 4.8 (1.5) in group E versus 6.6 (5.4) in group NE and at 72-96 h 4.5 (1.5) in group E versus 7.0 (4.0) in group NE. TIL domain scores were lower in group E for hyperosmolar therapy, targeted temperature management, and surgical management (cerebrospinal fluid drainage, evacuation, or decompressive craniectomy). The association between esmolol use after TBI and the reduction in ICP-directed interventions is consistent with an effect of beta-blockade on reduction of cerebral edema. Further research is necessary to determine causality and mechanism.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"5 1","pages":"982-987"},"PeriodicalIF":1.8000,"publicationDate":"2024-10-02","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491576/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Effect of Early Beta-Blockade with Esmolol on Therapy Intensity Level in Adults with Severe Traumatic Brain Injury.\",\"authors\":\"Thomas Baumer, George Higginbotham, Kati Hayes, Matt Thomas\",\"doi\":\"10.1089/neur.2024.0055\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Following severe traumatic brain injury (TBI), elevated catecholamine levels are associated with worsened secondary brain injury and poorer clinical outcomes. The mechanisms are uncertain but may include cerebral ischemia and blood-brain barrier disruption, with consequent cerebral edema manifesting as intracranial hypertension. Early beta-blockade (EBB) may mitigate these detrimental hyperadrenergic effects. Therapy Intensity Level (TIL) is a validated score that quantifies intracranial pressure (ICP)-lowering interventions, with higher TIL being a surrogate for more severe intracranial hypertension. In this <i>post hoc</i> secondary analysis of a dose-finding study of EBB with esmolol in adults with TBI, we compared summary TIL (TIL24) and domain TIL between patients who received esmolol and those who did not. The primary outcome was TIL24 for each 24-h epoch of the esmolol intervention period of 96 h. Baseline characteristics were comparable in the esmolol (E) and non-esmolol (NE) groups. Mean TIL24 was similar in both groups up to 48 h but then diverged. The mean (standard deviation) TIL24 score between 48 and 72 h was 4.8 (1.5) in group E versus 6.6 (5.4) in group NE and at 72-96 h 4.5 (1.5) in group E versus 7.0 (4.0) in group NE. TIL domain scores were lower in group E for hyperosmolar therapy, targeted temperature management, and surgical management (cerebrospinal fluid drainage, evacuation, or decompressive craniectomy). The association between esmolol use after TBI and the reduction in ICP-directed interventions is consistent with an effect of beta-blockade on reduction of cerebral edema. Further research is necessary to determine causality and mechanism.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"5 1\",\"pages\":\"982-987\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-10-02\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491576/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0055\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0055","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
The Effect of Early Beta-Blockade with Esmolol on Therapy Intensity Level in Adults with Severe Traumatic Brain Injury.
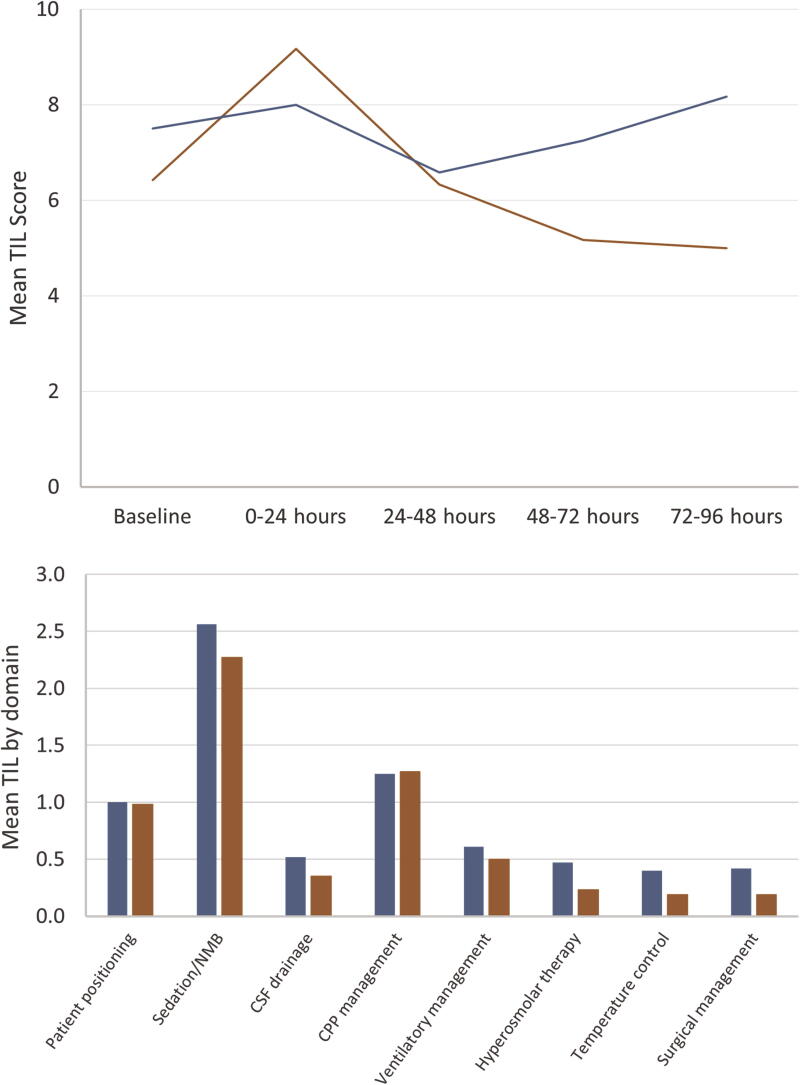
Following severe traumatic brain injury (TBI), elevated catecholamine levels are associated with worsened secondary brain injury and poorer clinical outcomes. The mechanisms are uncertain but may include cerebral ischemia and blood-brain barrier disruption, with consequent cerebral edema manifesting as intracranial hypertension. Early beta-blockade (EBB) may mitigate these detrimental hyperadrenergic effects. Therapy Intensity Level (TIL) is a validated score that quantifies intracranial pressure (ICP)-lowering interventions, with higher TIL being a surrogate for more severe intracranial hypertension. In this post hoc secondary analysis of a dose-finding study of EBB with esmolol in adults with TBI, we compared summary TIL (TIL24) and domain TIL between patients who received esmolol and those who did not. The primary outcome was TIL24 for each 24-h epoch of the esmolol intervention period of 96 h. Baseline characteristics were comparable in the esmolol (E) and non-esmolol (NE) groups. Mean TIL24 was similar in both groups up to 48 h but then diverged. The mean (standard deviation) TIL24 score between 48 and 72 h was 4.8 (1.5) in group E versus 6.6 (5.4) in group NE and at 72-96 h 4.5 (1.5) in group E versus 7.0 (4.0) in group NE. TIL domain scores were lower in group E for hyperosmolar therapy, targeted temperature management, and surgical management (cerebrospinal fluid drainage, evacuation, or decompressive craniectomy). The association between esmolol use after TBI and the reduction in ICP-directed interventions is consistent with an effect of beta-blockade on reduction of cerebral edema. Further research is necessary to determine causality and mechanism.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


