David Bark, Julia Basu, Dimitrios Toumpanakis, Johan Burwick Nyberg, Tomas Bjerner, Elham Rostami, David Fällmar
{"title":"在 CT 扫描中检测颅内出血的人工智能决策支持系统的临床影响。","authors":"David Bark, Julia Basu, Dimitrios Toumpanakis, Johan Burwick Nyberg, Tomas Bjerner, Elham Rostami, David Fällmar","doi":"10.1089/neur.2024.0017","DOIUrl":null,"url":null,"abstract":"<p><p>This study aimed to evaluate the predictive value and clinical impact of a clinically implemented artificial neural network software model. The software detects intracranial hemorrhage (ICH) from head computed tomography (CT) scans and artificial intelligence (AI)-identified positive cases are then annotated in the work list for early radiologist evaluation. The index test was AI detection by the program Zebra Medical Vision-HealthICH+. Radiologist-confirmed ICH was the reference standard. The study compared whether time benefits from using the AI model led to faster escalation of patient care or surgery within the first 24 h. A total of 2,306 patients were evaluated by the software, and 288 AI-positive cases were included. The AI tool had a positive predictive value of 0.823. There was, however, no significant time reduction when comparing the patients who required escalation of care and those who did not. There was also no significant time reduction in those who required acute surgery compared with those who did not. Among the individual patients with reduced time delay, no cases with evident clinical benefit were identified. Although the clinically implemented AI-based decision support system showed adequate predictive value in identifying ICH, there was no significant clinical benefit for the patients in our setting. While AI-assisted detection of ICH shows great promise from a technical perspective, there remains a need to evaluate the clinical impact and perform external validation across different settings.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"5 1","pages":"1009-1015"},"PeriodicalIF":1.8000,"publicationDate":"2024-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491571/pdf/","citationCount":"0","resultStr":"{\"title\":\"Clinical Impact of an AI Decision Support System for Detection of Intracranial Hemorrhage in CT Scans.\",\"authors\":\"David Bark, Julia Basu, Dimitrios Toumpanakis, Johan Burwick Nyberg, Tomas Bjerner, Elham Rostami, David Fällmar\",\"doi\":\"10.1089/neur.2024.0017\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>This study aimed to evaluate the predictive value and clinical impact of a clinically implemented artificial neural network software model. The software detects intracranial hemorrhage (ICH) from head computed tomography (CT) scans and artificial intelligence (AI)-identified positive cases are then annotated in the work list for early radiologist evaluation. The index test was AI detection by the program Zebra Medical Vision-HealthICH+. Radiologist-confirmed ICH was the reference standard. The study compared whether time benefits from using the AI model led to faster escalation of patient care or surgery within the first 24 h. A total of 2,306 patients were evaluated by the software, and 288 AI-positive cases were included. The AI tool had a positive predictive value of 0.823. There was, however, no significant time reduction when comparing the patients who required escalation of care and those who did not. There was also no significant time reduction in those who required acute surgery compared with those who did not. Among the individual patients with reduced time delay, no cases with evident clinical benefit were identified. Although the clinically implemented AI-based decision support system showed adequate predictive value in identifying ICH, there was no significant clinical benefit for the patients in our setting. While AI-assisted detection of ICH shows great promise from a technical perspective, there remains a need to evaluate the clinical impact and perform external validation across different settings.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"5 1\",\"pages\":\"1009-1015\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-10-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11491571/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0017\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0017","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
引用次数: 0
摘要
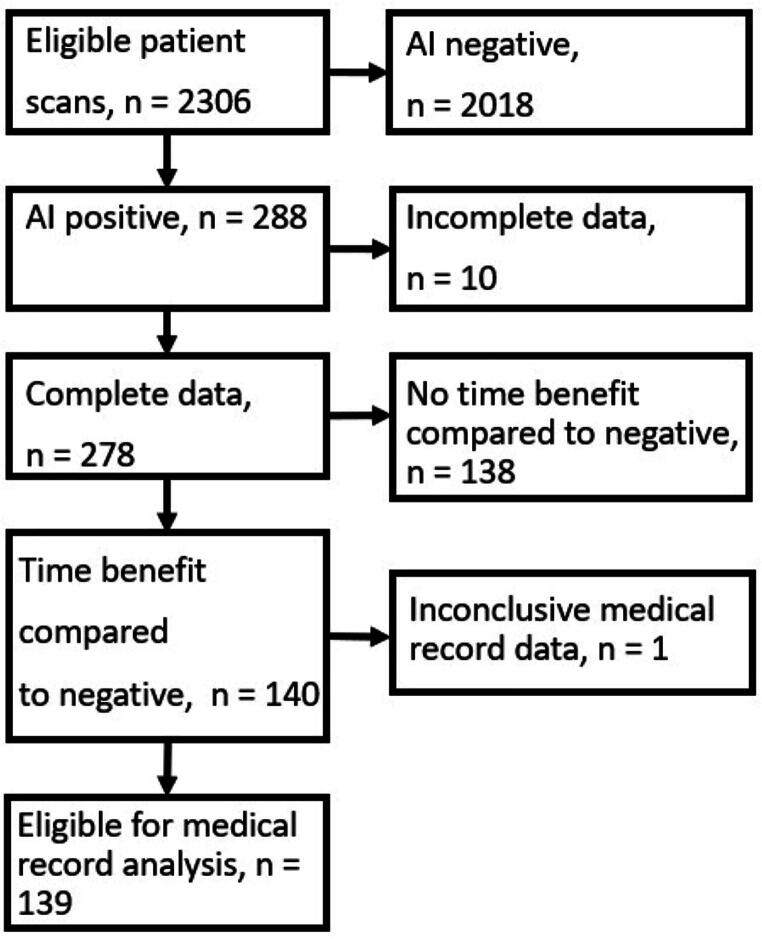
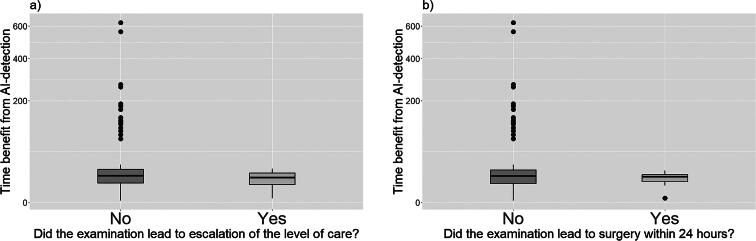
本研究旨在评估临床实施的人工神经网络软件模型的预测价值和临床影响。该软件从头部计算机断层扫描(CT)中检测颅内出血(ICH),然后将人工智能(AI)识别的阳性病例注释在工作列表中,供放射科医生进行早期评估。指标测试是由 Zebra Medical Vision-HealthICH+ 程序进行人工智能检测。放射科医生确认的 ICH 为参考标准。研究比较了使用人工智能模型是否能在24小时内更快地升级患者护理或手术。软件共评估了2306名患者,其中人工智能阳性病例288例。人工智能工具的阳性预测值为 0.823。不过,需要升级护理的患者与不需要升级护理的患者相比,时间并没有明显缩短。需要急性手术的患者与不需要急性手术的患者相比,时间也没有明显缩短。在时间延迟缩短的个别患者中,没有发现有明显临床获益的病例。虽然临床实施的人工智能决策支持系统在识别 ICH 方面显示出足够的预测价值,但在我们的环境中,患者并没有明显的临床获益。虽然从技术角度来看,人工智能辅助检测 ICH 显示出了巨大的前景,但仍有必要评估其临床影响,并在不同环境下进行外部验证。
Clinical Impact of an AI Decision Support System for Detection of Intracranial Hemorrhage in CT Scans.
This study aimed to evaluate the predictive value and clinical impact of a clinically implemented artificial neural network software model. The software detects intracranial hemorrhage (ICH) from head computed tomography (CT) scans and artificial intelligence (AI)-identified positive cases are then annotated in the work list for early radiologist evaluation. The index test was AI detection by the program Zebra Medical Vision-HealthICH+. Radiologist-confirmed ICH was the reference standard. The study compared whether time benefits from using the AI model led to faster escalation of patient care or surgery within the first 24 h. A total of 2,306 patients were evaluated by the software, and 288 AI-positive cases were included. The AI tool had a positive predictive value of 0.823. There was, however, no significant time reduction when comparing the patients who required escalation of care and those who did not. There was also no significant time reduction in those who required acute surgery compared with those who did not. Among the individual patients with reduced time delay, no cases with evident clinical benefit were identified. Although the clinically implemented AI-based decision support system showed adequate predictive value in identifying ICH, there was no significant clinical benefit for the patients in our setting. While AI-assisted detection of ICH shows great promise from a technical perspective, there remains a need to evaluate the clinical impact and perform external validation across different settings.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


