{"title":"肩胛下肌与小结节之间的夹层导致的急性不可恢复性肩关节前脱位:病例报告。","authors":"Nazim Sifi, Ahmad Madani, Mahdi Zeghdoud","doi":"10.20408/jti.2024.0044","DOIUrl":null,"url":null,"abstract":"<p><p>Efforts to reduce an anterior shoulder dislocation can fail due to numerous mechanical obstructions caused by soft tissue interposition (long head of the biceps, rotator cuff muscles, labrum, musculocutaneous nerve) and/or bony elements (displaced fragment of a greater tuberosity or glenoid fracture, bone impaction such as a Hill-Sachs lesion fixed on the glenoid rim, a bony Bankart lesion). Herein, we report the case of a 35-year-old man who sustained an anterior shoulder fracture-dislocation of his left shoulder after a fall. Despite a postreduction radiological examination that appeared misleadingly reassuring, subtle signs of persistent subluxation raised concerns. A computed tomography (CT) scan revealed subscapularis muscle entrapment along with avulsion of its bony insertion from the lesser tuberosity of the humerus, and a comminuted avulsion fracture of the greater tuberosity of the humerus. The patient underwent surgery using a deltopectoral approach. This involved releasing the entrapped subscapularis muscle and fixing the two fractured fragments. The lesser tuberosity was reduced and secured with two cannulated screws, and the comminuted fragment of the greater tuberosity was reattached using transosseous sutures. At 12-month follow-up, the patient achieved a Constant-Murley score of 85 of 100, with limitation in internal rotation at L3 but no signs of instability or new dislocation episode. This case underscores the importance of confirming shoulder reduction on at least two orthogonal views and paying close attention to the patient's feedback about sensation in their shoulder. Additionally, it highlights the utility of CT or magnetic resonance imaging scans if doubt exists about the integrity of the reduction.</p>","PeriodicalId":52698,"journal":{"name":"Journal of Trauma and Injury","volume":" ","pages":"38-43"},"PeriodicalIF":0.2000,"publicationDate":"2025-03-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968308/pdf/","citationCount":"0","resultStr":"{\"title\":\"Acute irreducible anterior shoulder dislocation due to interposition of the subscapularis muscle and the lesser tuberosity: a case report.\",\"authors\":\"Nazim Sifi, Ahmad Madani, Mahdi Zeghdoud\",\"doi\":\"10.20408/jti.2024.0044\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Efforts to reduce an anterior shoulder dislocation can fail due to numerous mechanical obstructions caused by soft tissue interposition (long head of the biceps, rotator cuff muscles, labrum, musculocutaneous nerve) and/or bony elements (displaced fragment of a greater tuberosity or glenoid fracture, bone impaction such as a Hill-Sachs lesion fixed on the glenoid rim, a bony Bankart lesion). Herein, we report the case of a 35-year-old man who sustained an anterior shoulder fracture-dislocation of his left shoulder after a fall. Despite a postreduction radiological examination that appeared misleadingly reassuring, subtle signs of persistent subluxation raised concerns. A computed tomography (CT) scan revealed subscapularis muscle entrapment along with avulsion of its bony insertion from the lesser tuberosity of the humerus, and a comminuted avulsion fracture of the greater tuberosity of the humerus. The patient underwent surgery using a deltopectoral approach. This involved releasing the entrapped subscapularis muscle and fixing the two fractured fragments. The lesser tuberosity was reduced and secured with two cannulated screws, and the comminuted fragment of the greater tuberosity was reattached using transosseous sutures. At 12-month follow-up, the patient achieved a Constant-Murley score of 85 of 100, with limitation in internal rotation at L3 but no signs of instability or new dislocation episode. This case underscores the importance of confirming shoulder reduction on at least two orthogonal views and paying close attention to the patient's feedback about sensation in their shoulder. Additionally, it highlights the utility of CT or magnetic resonance imaging scans if doubt exists about the integrity of the reduction.</p>\",\"PeriodicalId\":52698,\"journal\":{\"name\":\"Journal of Trauma and Injury\",\"volume\":\" \",\"pages\":\"38-43\"},\"PeriodicalIF\":0.2000,\"publicationDate\":\"2025-03-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11968308/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Trauma and Injury\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.20408/jti.2024.0044\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/21 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Trauma and Injury","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.20408/jti.2024.0044","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/21 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Acute irreducible anterior shoulder dislocation due to interposition of the subscapularis muscle and the lesser tuberosity: a case report.
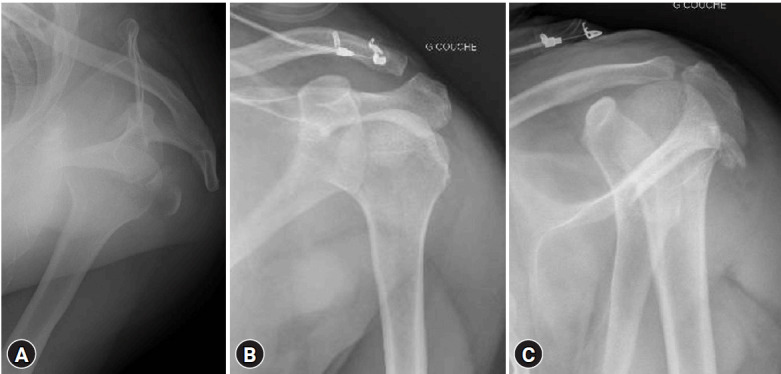
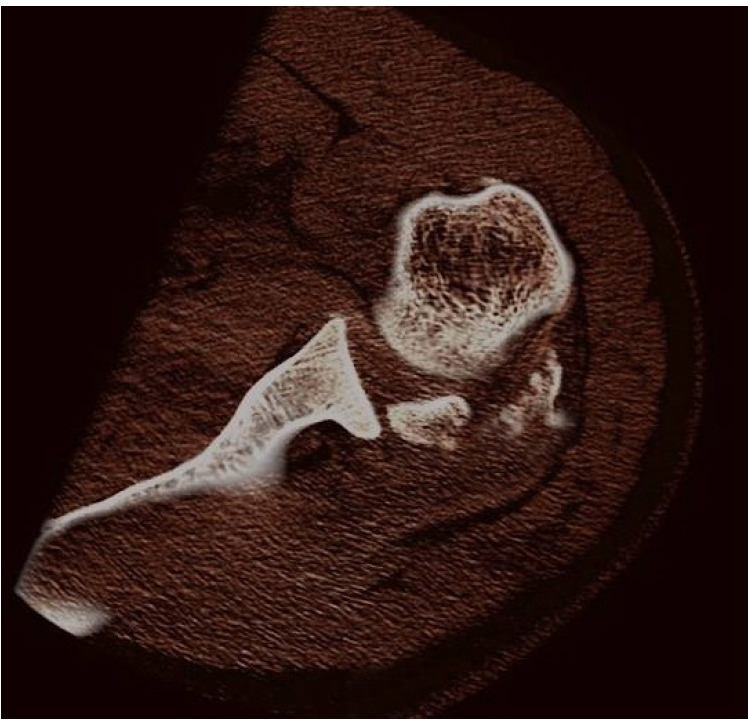
Efforts to reduce an anterior shoulder dislocation can fail due to numerous mechanical obstructions caused by soft tissue interposition (long head of the biceps, rotator cuff muscles, labrum, musculocutaneous nerve) and/or bony elements (displaced fragment of a greater tuberosity or glenoid fracture, bone impaction such as a Hill-Sachs lesion fixed on the glenoid rim, a bony Bankart lesion). Herein, we report the case of a 35-year-old man who sustained an anterior shoulder fracture-dislocation of his left shoulder after a fall. Despite a postreduction radiological examination that appeared misleadingly reassuring, subtle signs of persistent subluxation raised concerns. A computed tomography (CT) scan revealed subscapularis muscle entrapment along with avulsion of its bony insertion from the lesser tuberosity of the humerus, and a comminuted avulsion fracture of the greater tuberosity of the humerus. The patient underwent surgery using a deltopectoral approach. This involved releasing the entrapped subscapularis muscle and fixing the two fractured fragments. The lesser tuberosity was reduced and secured with two cannulated screws, and the comminuted fragment of the greater tuberosity was reattached using transosseous sutures. At 12-month follow-up, the patient achieved a Constant-Murley score of 85 of 100, with limitation in internal rotation at L3 but no signs of instability or new dislocation episode. This case underscores the importance of confirming shoulder reduction on at least two orthogonal views and paying close attention to the patient's feedback about sensation in their shoulder. Additionally, it highlights the utility of CT or magnetic resonance imaging scans if doubt exists about the integrity of the reduction.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


