Madeleine Carroll, Nensi Ruzgar, Maíra Fedatto, Kurt Schultz, Maija Cheung
{"title":"把钱拿出来1995年至2019年美国全球卫生资金分析。","authors":"Madeleine Carroll, Nensi Ruzgar, Maíra Fedatto, Kurt Schultz, Maija Cheung","doi":"10.7189/jogh.14.04173","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Historically, the US has been the largest contributor to development assistance for health (DAH), although its allocation has shifted in response to outside forces. This included, for example, the establishment of the Millennium Development Goals (MDGs) in 2000, which emphasised child mortality, maternal health, HIV/AIDS, and malaria. This led to funds being earmarked for disease-specific interventions rather than health system strengthening (HSS). In 2007, the World Health Organization (WHO) published six health system building blocks, representing essential components of strong health systems. In 2015, the MDGs were replaced by the Sustainable Development Goals (SDGs), which emphasised capacity-building as opposed to specific health problems. The Lancet Commission on Global Surgery, meanwhile, highlighted surgical capacity building as essential to achieving Universal Health Coverage (UHC). Given the renewed emphasis on a comprehensive approach rather than disease-specific interventions, one might anticipate the US aligning with this rhetoric in its allocation of DAH. However, we hypothesise that this is not the case.</p><p><strong>Methods: </strong>We queried the Organization for Economic Co-operation and Development (OECD) database for allocation of US DAH to low- and middle-income countries between 1995 and 2019, thereby excluding data after 2019 to avoid the influence of the coronavirus disease 2019 pandemic. OECD entries were assigned to health systems strengthening (HSS) or disease-specific interventions categories. The WHO building blocks were used as a framework for health systems strengthening.</p><p><strong>Results: </strong>From 1995 to 1999, US DAH allocated to HSS decreased from 42% to 34%. The allocation decreased further from 34% in 2000 to 4% in 2007; correspondingly, DAH allocated to disease-specific interventions increased from 67% to 96%. Between 2008 and 2019, the distribution of US DAH remained relatively stable, with funds allocated to HSS versus disease-specific interventions ranging from 3-12% and 88-98% respectively.</p><p><strong>Conclusions: </strong>While total US DAH contributions in the 1990s and early 2000s were significantly lower compared to the decade that followed, the distribution of these funds was more evenly divided between HSS and disease-specific interventions. Despite attempts by the WHO and United Nations to redirect attention to HSS as the path to achieving UHC, the US continues to largely support disease-specific interventions and overlook the importance of HSS, including surgical capacity building.</p>","PeriodicalId":48734,"journal":{"name":"Journal of Global Health","volume":"14 ","pages":"04173"},"PeriodicalIF":4.3000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11505566/pdf/","citationCount":"0","resultStr":"{\"title\":\"'Show me the money': An analysis of US global health funding from 1995 to 2019.\",\"authors\":\"Madeleine Carroll, Nensi Ruzgar, Maíra Fedatto, Kurt Schultz, Maija Cheung\",\"doi\":\"10.7189/jogh.14.04173\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Historically, the US has been the largest contributor to development assistance for health (DAH), although its allocation has shifted in response to outside forces. This included, for example, the establishment of the Millennium Development Goals (MDGs) in 2000, which emphasised child mortality, maternal health, HIV/AIDS, and malaria. This led to funds being earmarked for disease-specific interventions rather than health system strengthening (HSS). In 2007, the World Health Organization (WHO) published six health system building blocks, representing essential components of strong health systems. In 2015, the MDGs were replaced by the Sustainable Development Goals (SDGs), which emphasised capacity-building as opposed to specific health problems. The Lancet Commission on Global Surgery, meanwhile, highlighted surgical capacity building as essential to achieving Universal Health Coverage (UHC). Given the renewed emphasis on a comprehensive approach rather than disease-specific interventions, one might anticipate the US aligning with this rhetoric in its allocation of DAH. However, we hypothesise that this is not the case.</p><p><strong>Methods: </strong>We queried the Organization for Economic Co-operation and Development (OECD) database for allocation of US DAH to low- and middle-income countries between 1995 and 2019, thereby excluding data after 2019 to avoid the influence of the coronavirus disease 2019 pandemic. OECD entries were assigned to health systems strengthening (HSS) or disease-specific interventions categories. The WHO building blocks were used as a framework for health systems strengthening.</p><p><strong>Results: </strong>From 1995 to 1999, US DAH allocated to HSS decreased from 42% to 34%. The allocation decreased further from 34% in 2000 to 4% in 2007; correspondingly, DAH allocated to disease-specific interventions increased from 67% to 96%. Between 2008 and 2019, the distribution of US DAH remained relatively stable, with funds allocated to HSS versus disease-specific interventions ranging from 3-12% and 88-98% respectively.</p><p><strong>Conclusions: </strong>While total US DAH contributions in the 1990s and early 2000s were significantly lower compared to the decade that followed, the distribution of these funds was more evenly divided between HSS and disease-specific interventions. Despite attempts by the WHO and United Nations to redirect attention to HSS as the path to achieving UHC, the US continues to largely support disease-specific interventions and overlook the importance of HSS, including surgical capacity building.</p>\",\"PeriodicalId\":48734,\"journal\":{\"name\":\"Journal of Global Health\",\"volume\":\"14 \",\"pages\":\"04173\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11505566/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Global Health\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.7189/jogh.14.04173\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Global Health","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.7189/jogh.14.04173","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"PUBLIC, ENVIRONMENTAL & OCCUPATIONAL HEALTH","Score":null,"Total":0}
'Show me the money': An analysis of US global health funding from 1995 to 2019.
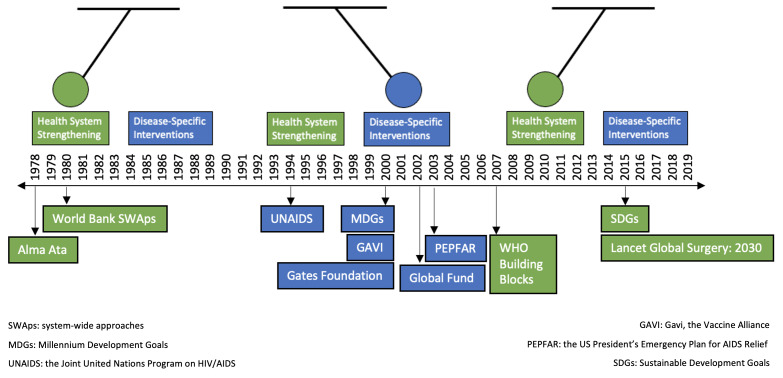
Background: Historically, the US has been the largest contributor to development assistance for health (DAH), although its allocation has shifted in response to outside forces. This included, for example, the establishment of the Millennium Development Goals (MDGs) in 2000, which emphasised child mortality, maternal health, HIV/AIDS, and malaria. This led to funds being earmarked for disease-specific interventions rather than health system strengthening (HSS). In 2007, the World Health Organization (WHO) published six health system building blocks, representing essential components of strong health systems. In 2015, the MDGs were replaced by the Sustainable Development Goals (SDGs), which emphasised capacity-building as opposed to specific health problems. The Lancet Commission on Global Surgery, meanwhile, highlighted surgical capacity building as essential to achieving Universal Health Coverage (UHC). Given the renewed emphasis on a comprehensive approach rather than disease-specific interventions, one might anticipate the US aligning with this rhetoric in its allocation of DAH. However, we hypothesise that this is not the case.
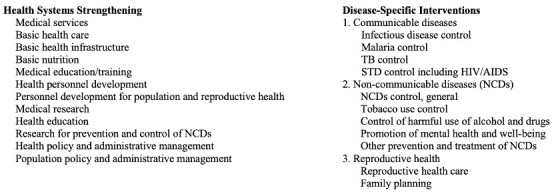
Methods: We queried the Organization for Economic Co-operation and Development (OECD) database for allocation of US DAH to low- and middle-income countries between 1995 and 2019, thereby excluding data after 2019 to avoid the influence of the coronavirus disease 2019 pandemic. OECD entries were assigned to health systems strengthening (HSS) or disease-specific interventions categories. The WHO building blocks were used as a framework for health systems strengthening.
Results: From 1995 to 1999, US DAH allocated to HSS decreased from 42% to 34%. The allocation decreased further from 34% in 2000 to 4% in 2007; correspondingly, DAH allocated to disease-specific interventions increased from 67% to 96%. Between 2008 and 2019, the distribution of US DAH remained relatively stable, with funds allocated to HSS versus disease-specific interventions ranging from 3-12% and 88-98% respectively.
Conclusions: While total US DAH contributions in the 1990s and early 2000s were significantly lower compared to the decade that followed, the distribution of these funds was more evenly divided between HSS and disease-specific interventions. Despite attempts by the WHO and United Nations to redirect attention to HSS as the path to achieving UHC, the US continues to largely support disease-specific interventions and overlook the importance of HSS, including surgical capacity building.
期刊介绍:
Journal of Global Health is a peer-reviewed journal published by the Edinburgh University Global Health Society, a not-for-profit organization registered in the UK. We publish editorials, news, viewpoints, original research and review articles in two issues per year.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


