Ashokkumar Singaravelu, Cathleen McCarrick, Shirley Potter, Ronan A. Cahill
{"title":"在乳房和头颈部重建中使用吲哚青绿荧光血管造影术进行术中皮瓣灌注评估的临床和成本效益:系统综述与元分析》。","authors":"Ashokkumar Singaravelu, Cathleen McCarrick, Shirley Potter, Ronan A. Cahill","doi":"10.1002/micr.31250","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Indocyanine green fluorescence angiography (ICGFA) is gaining popularity for the assessment of reconstructive flap perfusion intraoperatively. This study analyses the literature with a focus on its clinical efficacy and cost-effectiveness across various plastic and reconstructive surgery procedures.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A systematic review was conducted in accordance with PRISMA guidelines on published studies in English comparing ICGFA with standard clinical assessment for flap perfusion. Meta-analysis concerned perfusion-related complications and cost data.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Twenty-five studies met the inclusion criteria, of which two were randomized controlled trials (RCTs) and four were prospective cohort studies. Twenty-one studies were AHRQ Standard ‘Good’; however, the overall level of evidence remains low. ICGFA was predominantly performed in breast surgeries (<i>n</i> = 3310) and head and neck reconstruction (<i>n</i> = 701) albeit with inconsistency in protocols and predominantly subjective interpretations (only five studies utilized objective thresholds). In breast surgery, meta-analysis demonstrated significant reductions in mastectomy skin flap necrosis (odds ratio (OR) 0.58, <i>p</i> < 0.0001), fat necrosis (OR 0.31, <i>p</i> < 0.001), infection (OR 0.66, <i>p</i> = 0.02), and re-operation (OR 0.40, <i>p</i> < 0.0001), but no significant decrease in total or partial flap loss (OR 0.78, <i>p</i> = 0.57/OR 0.87, <i>p</i> = 0.56, respectively) or increase in dehiscence (OR 1.55, <i>p</i> = 0.11). In head and neck surgery, ICGFA significantly decreased total flap loss (OR 0.47, <i>p</i> = 0.04), although not partial flap loss (OR 0.37, <i>p</i> = 0.13) and reoperation (OR 0.92, <i>p</i> = 0.73). Lower limb (<i>n</i> = 104) and abdominal wall (<i>n</i> = 95) reconstructive surgeries were much less studied with no significant ICGFA impact. Seven studies reported cost savings with flap surgeries and breast reconstructions, although study heterogeneity precluded meta-analysis.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>ICGFA appears to be a useful, cost-effective tool to identify otherwise unsuspected hypoperfusion in breast and head and neck reconstruction. There is a clear need for standardization, however, to avoid bias. Further RCTs are necessary to solidify these promising clinical findings.</p>\n </section>\n </div>","PeriodicalId":18600,"journal":{"name":"Microsurgery","volume":"44 8","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-10-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/micr.31250","citationCount":"0","resultStr":"{\"title\":\"Clinical and Cost-Effectiveness of Intraoperative Flap Perfusion Assessment With Indocyanine Green Fluorescence Angiography in Breast and Head and Neck Reconstructions: A Systematic Review and Meta-Analysis\",\"authors\":\"Ashokkumar Singaravelu, Cathleen McCarrick, Shirley Potter, Ronan A. Cahill\",\"doi\":\"10.1002/micr.31250\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Indocyanine green fluorescence angiography (ICGFA) is gaining popularity for the assessment of reconstructive flap perfusion intraoperatively. This study analyses the literature with a focus on its clinical efficacy and cost-effectiveness across various plastic and reconstructive surgery procedures.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A systematic review was conducted in accordance with PRISMA guidelines on published studies in English comparing ICGFA with standard clinical assessment for flap perfusion. Meta-analysis concerned perfusion-related complications and cost data.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Twenty-five studies met the inclusion criteria, of which two were randomized controlled trials (RCTs) and four were prospective cohort studies. Twenty-one studies were AHRQ Standard ‘Good’; however, the overall level of evidence remains low. ICGFA was predominantly performed in breast surgeries (<i>n</i> = 3310) and head and neck reconstruction (<i>n</i> = 701) albeit with inconsistency in protocols and predominantly subjective interpretations (only five studies utilized objective thresholds). In breast surgery, meta-analysis demonstrated significant reductions in mastectomy skin flap necrosis (odds ratio (OR) 0.58, <i>p</i> < 0.0001), fat necrosis (OR 0.31, <i>p</i> < 0.001), infection (OR 0.66, <i>p</i> = 0.02), and re-operation (OR 0.40, <i>p</i> < 0.0001), but no significant decrease in total or partial flap loss (OR 0.78, <i>p</i> = 0.57/OR 0.87, <i>p</i> = 0.56, respectively) or increase in dehiscence (OR 1.55, <i>p</i> = 0.11). In head and neck surgery, ICGFA significantly decreased total flap loss (OR 0.47, <i>p</i> = 0.04), although not partial flap loss (OR 0.37, <i>p</i> = 0.13) and reoperation (OR 0.92, <i>p</i> = 0.73). Lower limb (<i>n</i> = 104) and abdominal wall (<i>n</i> = 95) reconstructive surgeries were much less studied with no significant ICGFA impact. Seven studies reported cost savings with flap surgeries and breast reconstructions, although study heterogeneity precluded meta-analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>ICGFA appears to be a useful, cost-effective tool to identify otherwise unsuspected hypoperfusion in breast and head and neck reconstruction. There is a clear need for standardization, however, to avoid bias. Further RCTs are necessary to solidify these promising clinical findings.</p>\\n </section>\\n </div>\",\"PeriodicalId\":18600,\"journal\":{\"name\":\"Microsurgery\",\"volume\":\"44 8\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-10-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/micr.31250\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Microsurgery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/micr.31250\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"SURGERY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Microsurgery","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/micr.31250","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"SURGERY","Score":null,"Total":0}
Clinical and Cost-Effectiveness of Intraoperative Flap Perfusion Assessment With Indocyanine Green Fluorescence Angiography in Breast and Head and Neck Reconstructions: A Systematic Review and Meta-Analysis
Background
Indocyanine green fluorescence angiography (ICGFA) is gaining popularity for the assessment of reconstructive flap perfusion intraoperatively. This study analyses the literature with a focus on its clinical efficacy and cost-effectiveness across various plastic and reconstructive surgery procedures.
Methods
A systematic review was conducted in accordance with PRISMA guidelines on published studies in English comparing ICGFA with standard clinical assessment for flap perfusion. Meta-analysis concerned perfusion-related complications and cost data.
Results
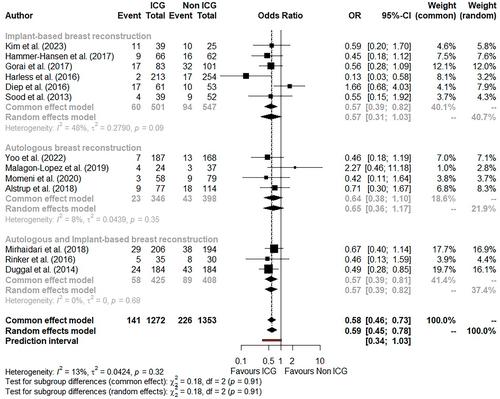
Twenty-five studies met the inclusion criteria, of which two were randomized controlled trials (RCTs) and four were prospective cohort studies. Twenty-one studies were AHRQ Standard ‘Good’; however, the overall level of evidence remains low. ICGFA was predominantly performed in breast surgeries (n = 3310) and head and neck reconstruction (n = 701) albeit with inconsistency in protocols and predominantly subjective interpretations (only five studies utilized objective thresholds). In breast surgery, meta-analysis demonstrated significant reductions in mastectomy skin flap necrosis (odds ratio (OR) 0.58, p < 0.0001), fat necrosis (OR 0.31, p < 0.001), infection (OR 0.66, p = 0.02), and re-operation (OR 0.40, p < 0.0001), but no significant decrease in total or partial flap loss (OR 0.78, p = 0.57/OR 0.87, p = 0.56, respectively) or increase in dehiscence (OR 1.55, p = 0.11). In head and neck surgery, ICGFA significantly decreased total flap loss (OR 0.47, p = 0.04), although not partial flap loss (OR 0.37, p = 0.13) and reoperation (OR 0.92, p = 0.73). Lower limb (n = 104) and abdominal wall (n = 95) reconstructive surgeries were much less studied with no significant ICGFA impact. Seven studies reported cost savings with flap surgeries and breast reconstructions, although study heterogeneity precluded meta-analysis.
Conclusions
ICGFA appears to be a useful, cost-effective tool to identify otherwise unsuspected hypoperfusion in breast and head and neck reconstruction. There is a clear need for standardization, however, to avoid bias. Further RCTs are necessary to solidify these promising clinical findings.
期刊介绍:
Microsurgery is an international and interdisciplinary publication of original contributions concerning surgery under microscopic magnification. Microsurgery publishes clinical studies, research papers, invited articles, relevant reviews, and other scholarly works from all related fields including orthopaedic surgery, otolaryngology, pediatric surgery, plastic surgery, urology, and vascular surgery.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:



