Chenglong Yu, Pradeep Natarajan, Aniruddh P Patel, Harpreet S Bhatia, Amit V Khera, Johannes T Neumann, Sotirios Tsimikas, Rory Wolfe, Stephen J Nicholls, Christopher M Reid, Sophia Zoungas, Andrew M Tonkin, John J McNeil, Paul Lacaze
{"title":"多基因风险、阿司匹林和冠心病一级预防。","authors":"Chenglong Yu, Pradeep Natarajan, Aniruddh P Patel, Harpreet S Bhatia, Amit V Khera, Johannes T Neumann, Sotirios Tsimikas, Rory Wolfe, Stephen J Nicholls, Christopher M Reid, Sophia Zoungas, Andrew M Tonkin, John J McNeil, Paul Lacaze","doi":"10.1093/ehjcvp/pvae085","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>Recent aspirin primary prevention trials failed to identify a net benefit of aspirin for preventing cardiovascular disease vs. the harms of bleeding. This study aimed to investigate whether a high-risk subgroup, individuals with elevated genetic predisposition to coronary artery disease (CAD), might derive more benefit than harm with aspirin, compared to those with lower genetic risk.</p><p><strong>Methods and results: </strong>We performed genetic risk stratification of the Aspirin in Reducing Events in the Elderly (ASPREE) randomized controlled trial using a CAD polygenic risk score (GPSMult). For 12 031 genotyped participants (5974 aspirin, 6057 placebo) overall, we stratified them by GPSMult quintiles (q1-5), then examined risk of CAD (composite of myocardial infarction and coronary heart disease death) and bleeding events using Cox models. During a median 4.6 years of follow-up with randomization to 100 mg/day aspirin vs. placebo, 234 (1.9%) participants had CAD and 373 (3.1%) had bleeding events. In the overall cohort, aspirin resulted in higher bleeding risk [adjusted Hazard ratio (aHR) = 1.30 (1.06-1.61), P = 0.01] but no significant CAD reduction [aHR = 0.84 (0.64-1.09), P = 0.19]. However, among the highest quintile of polygenic risk (q5, top 20% of the GPSMult distribution), there was a 47% reduction in risk of CAD events with aspirin [aHR = 0.53 (0.31-0.90), P = 0.02] without increased bleeding risk [aHR = 1.05 (0.60-1.82), P = 0.88]. Interaction between the GPSMult and aspirin was significant for CAD (q5 vs. q1, P = 0.02) but not bleeding (P = 0.80).</p><p><strong>Conclusion: </strong>The balance between net benefit and harm on aspirin in the primary prevention setting shifts favourably in individuals with an elevated genetic predisposition.</p>","PeriodicalId":11982,"journal":{"name":"European Heart Journal - Cardiovascular Pharmacotherapy","volume":" ","pages":"84-91"},"PeriodicalIF":6.1000,"publicationDate":"2025-02-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11805692/pdf/","citationCount":"0","resultStr":"{\"title\":\"Polygenic risk, aspirin, and primary prevention of coronary artery disease.\",\"authors\":\"Chenglong Yu, Pradeep Natarajan, Aniruddh P Patel, Harpreet S Bhatia, Amit V Khera, Johannes T Neumann, Sotirios Tsimikas, Rory Wolfe, Stephen J Nicholls, Christopher M Reid, Sophia Zoungas, Andrew M Tonkin, John J McNeil, Paul Lacaze\",\"doi\":\"10.1093/ehjcvp/pvae085\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>Recent aspirin primary prevention trials failed to identify a net benefit of aspirin for preventing cardiovascular disease vs. the harms of bleeding. This study aimed to investigate whether a high-risk subgroup, individuals with elevated genetic predisposition to coronary artery disease (CAD), might derive more benefit than harm with aspirin, compared to those with lower genetic risk.</p><p><strong>Methods and results: </strong>We performed genetic risk stratification of the Aspirin in Reducing Events in the Elderly (ASPREE) randomized controlled trial using a CAD polygenic risk score (GPSMult). For 12 031 genotyped participants (5974 aspirin, 6057 placebo) overall, we stratified them by GPSMult quintiles (q1-5), then examined risk of CAD (composite of myocardial infarction and coronary heart disease death) and bleeding events using Cox models. During a median 4.6 years of follow-up with randomization to 100 mg/day aspirin vs. placebo, 234 (1.9%) participants had CAD and 373 (3.1%) had bleeding events. In the overall cohort, aspirin resulted in higher bleeding risk [adjusted Hazard ratio (aHR) = 1.30 (1.06-1.61), P = 0.01] but no significant CAD reduction [aHR = 0.84 (0.64-1.09), P = 0.19]. However, among the highest quintile of polygenic risk (q5, top 20% of the GPSMult distribution), there was a 47% reduction in risk of CAD events with aspirin [aHR = 0.53 (0.31-0.90), P = 0.02] without increased bleeding risk [aHR = 1.05 (0.60-1.82), P = 0.88]. Interaction between the GPSMult and aspirin was significant for CAD (q5 vs. q1, P = 0.02) but not bleeding (P = 0.80).</p><p><strong>Conclusion: </strong>The balance between net benefit and harm on aspirin in the primary prevention setting shifts favourably in individuals with an elevated genetic predisposition.</p>\",\"PeriodicalId\":11982,\"journal\":{\"name\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"volume\":\" \",\"pages\":\"84-91\"},\"PeriodicalIF\":6.1000,\"publicationDate\":\"2025-02-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11805692/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Heart Journal - Cardiovascular Pharmacotherapy\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1093/ehjcvp/pvae085\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Heart Journal - Cardiovascular Pharmacotherapy","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1093/ehjcvp/pvae085","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
Polygenic risk, aspirin, and primary prevention of coronary artery disease.
Aims: Recent aspirin primary prevention trials failed to identify a net benefit of aspirin for preventing cardiovascular disease vs. the harms of bleeding. This study aimed to investigate whether a high-risk subgroup, individuals with elevated genetic predisposition to coronary artery disease (CAD), might derive more benefit than harm with aspirin, compared to those with lower genetic risk.
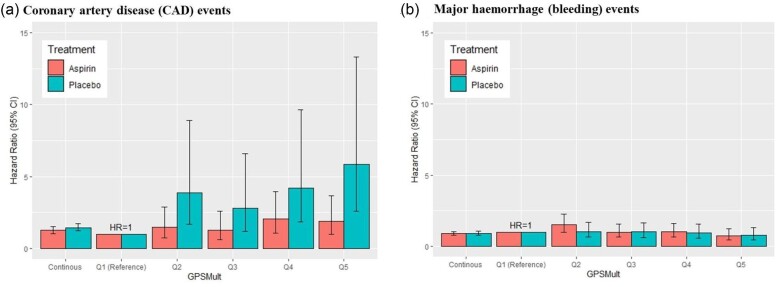
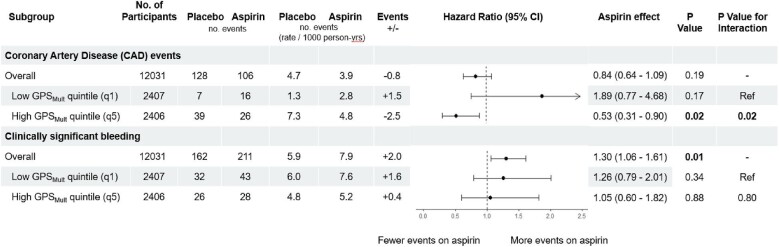
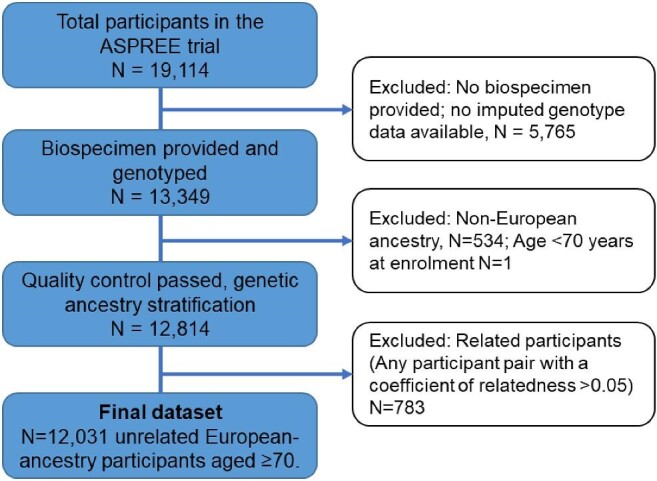
Methods and results: We performed genetic risk stratification of the Aspirin in Reducing Events in the Elderly (ASPREE) randomized controlled trial using a CAD polygenic risk score (GPSMult). For 12 031 genotyped participants (5974 aspirin, 6057 placebo) overall, we stratified them by GPSMult quintiles (q1-5), then examined risk of CAD (composite of myocardial infarction and coronary heart disease death) and bleeding events using Cox models. During a median 4.6 years of follow-up with randomization to 100 mg/day aspirin vs. placebo, 234 (1.9%) participants had CAD and 373 (3.1%) had bleeding events. In the overall cohort, aspirin resulted in higher bleeding risk [adjusted Hazard ratio (aHR) = 1.30 (1.06-1.61), P = 0.01] but no significant CAD reduction [aHR = 0.84 (0.64-1.09), P = 0.19]. However, among the highest quintile of polygenic risk (q5, top 20% of the GPSMult distribution), there was a 47% reduction in risk of CAD events with aspirin [aHR = 0.53 (0.31-0.90), P = 0.02] without increased bleeding risk [aHR = 1.05 (0.60-1.82), P = 0.88]. Interaction between the GPSMult and aspirin was significant for CAD (q5 vs. q1, P = 0.02) but not bleeding (P = 0.80).
Conclusion: The balance between net benefit and harm on aspirin in the primary prevention setting shifts favourably in individuals with an elevated genetic predisposition.
期刊介绍:
The European Heart Journal - Cardiovascular Pharmacotherapy (EHJ-CVP) is an international, peer-reviewed journal published in English, specifically dedicated to clinical cardiovascular pharmacology. EHJ-CVP publishes original articles focusing on clinical research involving both new and established drugs and methods, along with meta-analyses and topical reviews. The journal's primary aim is to enhance the pharmacological treatment of patients with cardiovascular disease by interpreting and integrating new scientific developments in this field.
While the emphasis is on clinical topics, EHJ-CVP also considers basic research articles from fields such as physiology and molecular biology that contribute to the understanding of cardiovascular drug therapy. These may include articles related to new drug development and evaluation, the physiological and pharmacological basis of drug action, metabolism, drug interactions, and side effects.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


