Yimeng Zhang, Pushpa Singh, Kavitha Ganapathy, Vijayan Suresh, Muhammad Ali Karamat, Jyoti Baharani, Srikanth Bellary
{"title":"持续葡萄糖监测对糖尿病患者和透析终末期肾病患者的疗效:系统综述。","authors":"Yimeng Zhang, Pushpa Singh, Kavitha Ganapathy, Vijayan Suresh, Muhammad Ali Karamat, Jyoti Baharani, Srikanth Bellary","doi":"10.1186/s12882-024-03763-z","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Patients with diabetes on dialysis experience wide variations in glucose levels and an increased risk of hypoglycaemia. Due to the inaccuracies of HbA1c in dialysis patients, JBDS-IP and KDIGO recommend the use of continuous glucose monitoring (CGM). We conducted a systematic review to examine the current evidence for CGM use and its impact on clinical outcomes in patients with diabetes on dialysis.</p><p><strong>Methods: </strong>A search of MEDLINE(R) ALL, Ovid Emcare, Journals@Ovid Full Text and Embase databases were conducted. Clinical or observational trials in adults with Type 1(T1D) or Type 2 (T2D) diabetes on dialysis and CGM intervention reporting on glycaemic outcomes were included.</p><p><strong>Results: </strong>Of the 936 citations identified, 49 duplicates were removed. 887 citations were screened by title and abstract. 9 full texts were reviewed and a further 7 excluded due to duplications or failure to meet to selection criteria. Data was extracted for 2 studies, both prospective before-and-after interventional studies with no control group. Joubert et al. (2015) showed results for 15 participants with T1D. Mean CGM glucose level decreased from 8.37mmol/L at baseline to 7.7mmol/L at the end of the CGM period (p < 0.05) while HbA1c decreased from 6.9 to 6.5% (p < 0.05) during the same period. Mean CGM was lower on dialysis days (7.68mmol/L vs. 7.8mmol/L, p < 0.05). Képénékian et al. (2014) reported on data from 29 T2D patients. Following a 3 month CGM-adapted insulin regimen, HbA1c decreased from 8.4% at baseline to 7.6% (p < 0.01) by the end of study. Mean CGM values decreased from 9.9mmol/L to 8.9mmol/L (p = 0.05) and the frequency of glucose values > 10mmol/L decreased from 41 to 30% (p < 0.05), without a significant increase in hypoglycaemia frequency. Both studies were deemed to be of 'good' quality.</p><p><strong>Conclusion: </strong>Evidence demonstrating the benefits of CGM in patients with diabetes receiving dialysis is lacking. There is a need for well-designed randomised controlled trials to ascertain the benefits of this technology in this patient group.</p><p><strong>Trail registration: </strong>PROSPERO registration number: CRD42023371635, https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=371635 .</p>","PeriodicalId":9089,"journal":{"name":"BMC Nephrology","volume":"25 1","pages":"379"},"PeriodicalIF":2.4000,"publicationDate":"2024-10-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515242/pdf/","citationCount":"0","resultStr":"{\"title\":\"Efficacy of continuous glucose monitoring in people living with diabetes and end stage kidney disease on dialysis: a systematic review.\",\"authors\":\"Yimeng Zhang, Pushpa Singh, Kavitha Ganapathy, Vijayan Suresh, Muhammad Ali Karamat, Jyoti Baharani, Srikanth Bellary\",\"doi\":\"10.1186/s12882-024-03763-z\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Patients with diabetes on dialysis experience wide variations in glucose levels and an increased risk of hypoglycaemia. Due to the inaccuracies of HbA1c in dialysis patients, JBDS-IP and KDIGO recommend the use of continuous glucose monitoring (CGM). We conducted a systematic review to examine the current evidence for CGM use and its impact on clinical outcomes in patients with diabetes on dialysis.</p><p><strong>Methods: </strong>A search of MEDLINE(R) ALL, Ovid Emcare, Journals@Ovid Full Text and Embase databases were conducted. Clinical or observational trials in adults with Type 1(T1D) or Type 2 (T2D) diabetes on dialysis and CGM intervention reporting on glycaemic outcomes were included.</p><p><strong>Results: </strong>Of the 936 citations identified, 49 duplicates were removed. 887 citations were screened by title and abstract. 9 full texts were reviewed and a further 7 excluded due to duplications or failure to meet to selection criteria. Data was extracted for 2 studies, both prospective before-and-after interventional studies with no control group. Joubert et al. (2015) showed results for 15 participants with T1D. Mean CGM glucose level decreased from 8.37mmol/L at baseline to 7.7mmol/L at the end of the CGM period (p < 0.05) while HbA1c decreased from 6.9 to 6.5% (p < 0.05) during the same period. Mean CGM was lower on dialysis days (7.68mmol/L vs. 7.8mmol/L, p < 0.05). Képénékian et al. (2014) reported on data from 29 T2D patients. Following a 3 month CGM-adapted insulin regimen, HbA1c decreased from 8.4% at baseline to 7.6% (p < 0.01) by the end of study. Mean CGM values decreased from 9.9mmol/L to 8.9mmol/L (p = 0.05) and the frequency of glucose values > 10mmol/L decreased from 41 to 30% (p < 0.05), without a significant increase in hypoglycaemia frequency. Both studies were deemed to be of 'good' quality.</p><p><strong>Conclusion: </strong>Evidence demonstrating the benefits of CGM in patients with diabetes receiving dialysis is lacking. There is a need for well-designed randomised controlled trials to ascertain the benefits of this technology in this patient group.</p><p><strong>Trail registration: </strong>PROSPERO registration number: CRD42023371635, https://www.crd.york.ac.uk/PROSPERO/display_record.php?RecordID=371635 .</p>\",\"PeriodicalId\":9089,\"journal\":{\"name\":\"BMC Nephrology\",\"volume\":\"25 1\",\"pages\":\"379\"},\"PeriodicalIF\":2.4000,\"publicationDate\":\"2024-10-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11515242/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Nephrology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12882-024-03763-z\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Nephrology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12882-024-03763-z","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Efficacy of continuous glucose monitoring in people living with diabetes and end stage kidney disease on dialysis: a systematic review.
Background: Patients with diabetes on dialysis experience wide variations in glucose levels and an increased risk of hypoglycaemia. Due to the inaccuracies of HbA1c in dialysis patients, JBDS-IP and KDIGO recommend the use of continuous glucose monitoring (CGM). We conducted a systematic review to examine the current evidence for CGM use and its impact on clinical outcomes in patients with diabetes on dialysis.
Methods: A search of MEDLINE(R) ALL, Ovid Emcare, Journals@Ovid Full Text and Embase databases were conducted. Clinical or observational trials in adults with Type 1(T1D) or Type 2 (T2D) diabetes on dialysis and CGM intervention reporting on glycaemic outcomes were included.
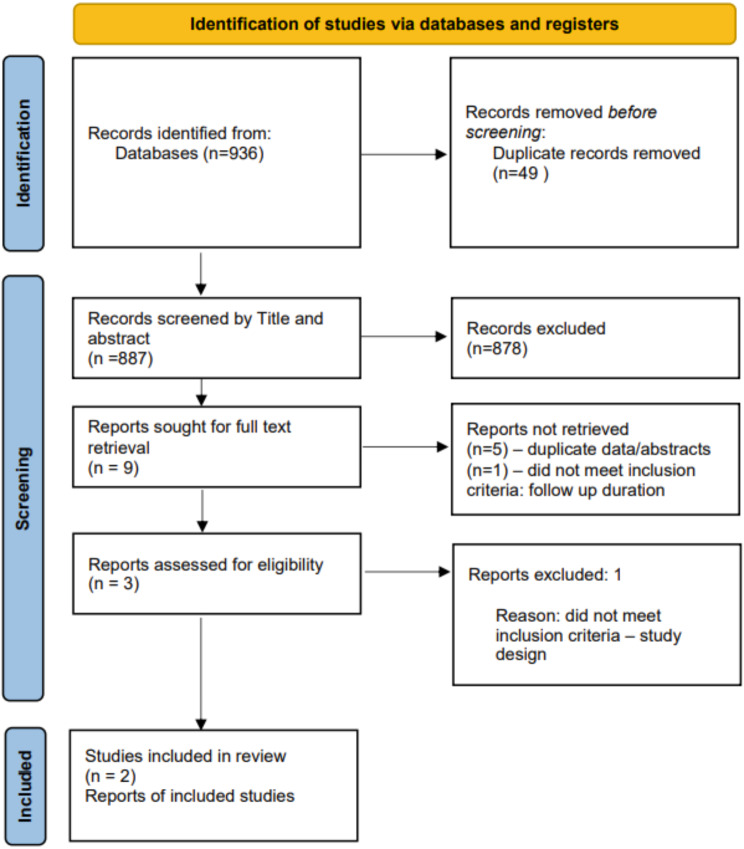
Results: Of the 936 citations identified, 49 duplicates were removed. 887 citations were screened by title and abstract. 9 full texts were reviewed and a further 7 excluded due to duplications or failure to meet to selection criteria. Data was extracted for 2 studies, both prospective before-and-after interventional studies with no control group. Joubert et al. (2015) showed results for 15 participants with T1D. Mean CGM glucose level decreased from 8.37mmol/L at baseline to 7.7mmol/L at the end of the CGM period (p < 0.05) while HbA1c decreased from 6.9 to 6.5% (p < 0.05) during the same period. Mean CGM was lower on dialysis days (7.68mmol/L vs. 7.8mmol/L, p < 0.05). Képénékian et al. (2014) reported on data from 29 T2D patients. Following a 3 month CGM-adapted insulin regimen, HbA1c decreased from 8.4% at baseline to 7.6% (p < 0.01) by the end of study. Mean CGM values decreased from 9.9mmol/L to 8.9mmol/L (p = 0.05) and the frequency of glucose values > 10mmol/L decreased from 41 to 30% (p < 0.05), without a significant increase in hypoglycaemia frequency. Both studies were deemed to be of 'good' quality.
Conclusion: Evidence demonstrating the benefits of CGM in patients with diabetes receiving dialysis is lacking. There is a need for well-designed randomised controlled trials to ascertain the benefits of this technology in this patient group.
期刊介绍:
BMC Nephrology is an open access journal publishing original peer-reviewed research articles in all aspects of the prevention, diagnosis and management of kidney and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


