Mehmet Orkun Sevik, Nimet Zeynep Tiras, Aslan Aykut, Didem Dizdar Yigit, Ozlem Sahin
{"title":"考虑到土耳其的报销问题,真实的新生血管性黄斑变性治疗:治疗失败后改用玻璃体内注射雷尼珠单抗或阿弗利贝赛普治疗一年的比较。","authors":"Mehmet Orkun Sevik, Nimet Zeynep Tiras, Aslan Aykut, Didem Dizdar Yigit, Ozlem Sahin","doi":"10.14744/nci.2024.75688","DOIUrl":null,"url":null,"abstract":"<p><strong>Objective: </strong>To compare one-year anatomical and functional results of switching to an on-label intravitreal anti-vascular endothelial growth factor (anti-VEGF) agent (intravitreal ranibizumab [IVR] or aflibercept [IVA]) after treatment failure with three loading doses of off-label intravitreal bevacizumab (IVB), which is mandatory in the treatment of neovascular age-related macular degeneration (nAMD) to get reimbursement from Social Security Institution in Turkiye.</p><p><strong>Methods: </strong>This comparative, real-life, retrospective cohort study included treatment-naïve nAMD patients treated starting with three loading doses of IVB, switched to three loading doses of IVR and IVA due to treatment failure after IVB loading, and followed up one year with a treat-and-extend (T&E) protocol with 2-week extension/shortening intervals. The primary outcomes were changes in best-corrected visual acuity (BCVA; logMAR) and central macular thickness (CMT, µm) one year after the switch, and the secondary outcomes were maximum treatment intervals, number of injections, and disease activity rates.</p><p><strong>Results: </strong>The mean age (72.9±8.2 and 72.2±6.7, p=0.677) and gender (60.0% and 47.4% females, p=0.398) were similar among the IVR (35 eyes/patients) and IVA (38 eyes/patients) groups. The median BCVA and CMT were significantly improved during the study period (p<0.001) with no significant intergroup differences. The ratio of 4-, 6-, 8-, 10-, and 12-week maximum treatment intervals were 28.6%, 17.1%, 14.3%, 8.6%, and 31.4% in the IVR, and 13.2%, 15.8%, 21.1%, 15.8%, and 34.2% in the IVA group (p=0.492). The median (IQR) number of injections in the IVA group (8 [7-9]) was significantly lower than the IVR group (9 [8-12]) during the one-year T&E period (p=0.026). The disease activity rates were 34.3% and 26.4% one month (p=0.610) and 37.1% and 21.1% one year (p=0.195) after the switch in IVR and IVA groups.</p><p><strong>Conclusion: </strong>This real-life comparison study indicates that, after the treatment failure with three loading doses of IVB, switching to either on-label anti-VEGF agent can be regarded as comparable considering functional and anatomical results. However, although maximum treatment intervals were not significantly different, fewer injections were required with aflibercept during the one-year T&E follow-up period.</p>","PeriodicalId":94347,"journal":{"name":"Northern clinics of Istanbul","volume":"11 5","pages":"451-459"},"PeriodicalIF":0.9000,"publicationDate":"2024-10-03","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487320/pdf/","citationCount":"0","resultStr":"{\"title\":\"Real-life neovascular AMD treatment considering reimbursement in Turkiye: One-year comparison of switching to intravitreal ranibizumab or aflibercept after treatment failure with three loading intravitreal bevacizumab injections.\",\"authors\":\"Mehmet Orkun Sevik, Nimet Zeynep Tiras, Aslan Aykut, Didem Dizdar Yigit, Ozlem Sahin\",\"doi\":\"10.14744/nci.2024.75688\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Objective: </strong>To compare one-year anatomical and functional results of switching to an on-label intravitreal anti-vascular endothelial growth factor (anti-VEGF) agent (intravitreal ranibizumab [IVR] or aflibercept [IVA]) after treatment failure with three loading doses of off-label intravitreal bevacizumab (IVB), which is mandatory in the treatment of neovascular age-related macular degeneration (nAMD) to get reimbursement from Social Security Institution in Turkiye.</p><p><strong>Methods: </strong>This comparative, real-life, retrospective cohort study included treatment-naïve nAMD patients treated starting with three loading doses of IVB, switched to three loading doses of IVR and IVA due to treatment failure after IVB loading, and followed up one year with a treat-and-extend (T&E) protocol with 2-week extension/shortening intervals. The primary outcomes were changes in best-corrected visual acuity (BCVA; logMAR) and central macular thickness (CMT, µm) one year after the switch, and the secondary outcomes were maximum treatment intervals, number of injections, and disease activity rates.</p><p><strong>Results: </strong>The mean age (72.9±8.2 and 72.2±6.7, p=0.677) and gender (60.0% and 47.4% females, p=0.398) were similar among the IVR (35 eyes/patients) and IVA (38 eyes/patients) groups. The median BCVA and CMT were significantly improved during the study period (p<0.001) with no significant intergroup differences. The ratio of 4-, 6-, 8-, 10-, and 12-week maximum treatment intervals were 28.6%, 17.1%, 14.3%, 8.6%, and 31.4% in the IVR, and 13.2%, 15.8%, 21.1%, 15.8%, and 34.2% in the IVA group (p=0.492). The median (IQR) number of injections in the IVA group (8 [7-9]) was significantly lower than the IVR group (9 [8-12]) during the one-year T&E period (p=0.026). The disease activity rates were 34.3% and 26.4% one month (p=0.610) and 37.1% and 21.1% one year (p=0.195) after the switch in IVR and IVA groups.</p><p><strong>Conclusion: </strong>This real-life comparison study indicates that, after the treatment failure with three loading doses of IVB, switching to either on-label anti-VEGF agent can be regarded as comparable considering functional and anatomical results. However, although maximum treatment intervals were not significantly different, fewer injections were required with aflibercept during the one-year T&E follow-up period.</p>\",\"PeriodicalId\":94347,\"journal\":{\"name\":\"Northern clinics of Istanbul\",\"volume\":\"11 5\",\"pages\":\"451-459\"},\"PeriodicalIF\":0.9000,\"publicationDate\":\"2024-10-03\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11487320/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Northern clinics of Istanbul\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.14744/nci.2024.75688\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Northern clinics of Istanbul","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.14744/nci.2024.75688","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"","JCRName":"","Score":null,"Total":0}
Real-life neovascular AMD treatment considering reimbursement in Turkiye: One-year comparison of switching to intravitreal ranibizumab or aflibercept after treatment failure with three loading intravitreal bevacizumab injections.
Objective: To compare one-year anatomical and functional results of switching to an on-label intravitreal anti-vascular endothelial growth factor (anti-VEGF) agent (intravitreal ranibizumab [IVR] or aflibercept [IVA]) after treatment failure with three loading doses of off-label intravitreal bevacizumab (IVB), which is mandatory in the treatment of neovascular age-related macular degeneration (nAMD) to get reimbursement from Social Security Institution in Turkiye.
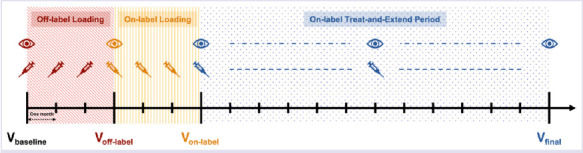
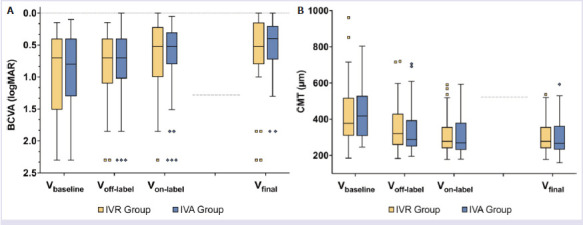
Methods: This comparative, real-life, retrospective cohort study included treatment-naïve nAMD patients treated starting with three loading doses of IVB, switched to three loading doses of IVR and IVA due to treatment failure after IVB loading, and followed up one year with a treat-and-extend (T&E) protocol with 2-week extension/shortening intervals. The primary outcomes were changes in best-corrected visual acuity (BCVA; logMAR) and central macular thickness (CMT, µm) one year after the switch, and the secondary outcomes were maximum treatment intervals, number of injections, and disease activity rates.
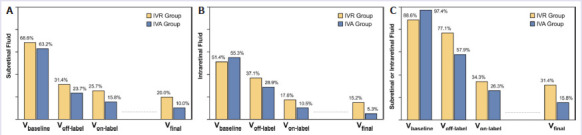
Results: The mean age (72.9±8.2 and 72.2±6.7, p=0.677) and gender (60.0% and 47.4% females, p=0.398) were similar among the IVR (35 eyes/patients) and IVA (38 eyes/patients) groups. The median BCVA and CMT were significantly improved during the study period (p<0.001) with no significant intergroup differences. The ratio of 4-, 6-, 8-, 10-, and 12-week maximum treatment intervals were 28.6%, 17.1%, 14.3%, 8.6%, and 31.4% in the IVR, and 13.2%, 15.8%, 21.1%, 15.8%, and 34.2% in the IVA group (p=0.492). The median (IQR) number of injections in the IVA group (8 [7-9]) was significantly lower than the IVR group (9 [8-12]) during the one-year T&E period (p=0.026). The disease activity rates were 34.3% and 26.4% one month (p=0.610) and 37.1% and 21.1% one year (p=0.195) after the switch in IVR and IVA groups.
Conclusion: This real-life comparison study indicates that, after the treatment failure with three loading doses of IVB, switching to either on-label anti-VEGF agent can be regarded as comparable considering functional and anatomical results. However, although maximum treatment intervals were not significantly different, fewer injections were required with aflibercept during the one-year T&E follow-up period.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


