Xingxing Li, Cuiyu Xie, Yangyang Wu, Weiwei Zhong, Yao Lu, Yuanhai Li
{"title":"在清醒直接喉镜检查中静脉注射纳布啡和右美托咪定联合吸入利多卡因气雾剂的比较:随机、双盲、安慰剂对照试验。","authors":"Xingxing Li, Cuiyu Xie, Yangyang Wu, Weiwei Zhong, Yao Lu, Yuanhai Li","doi":"10.1186/s13741-024-00461-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The airway should be thoroughly and accurately evaluated before anesthesia induction and endotracheal intubation. Awake direct laryngoscopy (ADL) can provide rapid, accurate, and intuitive airway assessment, especially for suspected difficult airways, and sometimes eliminates the need for fiberoptic intubation in some suspicious difficult airway cases. However, an optimal regimen has not been determined.</p><p><strong>Methods: </strong>In this double-blind, controlled study, prior to ADL, 60 patients scheduled for general anesthesia were randomly allocated to receive 0.75 μg/kg of dexmedetomidine (Dex group, n = 20), 0.15 mg/kg of nalbuphine (Nal group, n = 20), or a placebo (control group, n = 20) intravenously over 10 min. At the same time, all study subjects received nebulized lidocaine for 15 min. The primary outcome was patient tolerance as assessed by a 5-point ADL comfort score, while secondary outcomes included satisfaction, coughing, pain, nausea and vital signs.</p><p><strong>Results: </strong>Patients undergoing ADL in the Nal group had higher tolerance scores than those in the control and Dex groups [4 (3,4) vs. 3 (2,2.75), P < 0.017, and 4 (3,4) vs. 2 (2,2,75), P < 0.001, respectively] and higher satisfaction [7 (6,8) vs. 4 (3,5.75), P < 0.017, and 7 (6,8) vs. 5.5 (5,6), P < 0.001, respectively]. Additionally, the Nal group had significantly fewer adverse events, such as pain and nausea than the control and Dex groups. The sedation score and peripheral oxygen and saturation were significantly higher in the Nal group than in the Dex group, with no difference between the Nal and control groups (P < 0.001, P = 0.159, respectively).</p><p><strong>Conclusions: </strong>Intravenous nalbuphine in combination with lidocaine aerosol inhalation significantly improved patient tolerance and satisfaction while reducing nausea, coughing, pain, sedation, and SpO<sub>2</sub> levels during ADL.</p>","PeriodicalId":19764,"journal":{"name":"Perioperative Medicine","volume":"13 1","pages":"105"},"PeriodicalIF":2.1000,"publicationDate":"2024-10-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11490102/pdf/","citationCount":"0","resultStr":"{\"title\":\"Comparison of intravenous nalbuphine and dexmedetomidine in combination with lidocaine aerosol inhalation in awake direct laryngoscopy: a randomized, double-blind, placebo-controlled trial.\",\"authors\":\"Xingxing Li, Cuiyu Xie, Yangyang Wu, Weiwei Zhong, Yao Lu, Yuanhai Li\",\"doi\":\"10.1186/s13741-024-00461-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The airway should be thoroughly and accurately evaluated before anesthesia induction and endotracheal intubation. Awake direct laryngoscopy (ADL) can provide rapid, accurate, and intuitive airway assessment, especially for suspected difficult airways, and sometimes eliminates the need for fiberoptic intubation in some suspicious difficult airway cases. However, an optimal regimen has not been determined.</p><p><strong>Methods: </strong>In this double-blind, controlled study, prior to ADL, 60 patients scheduled for general anesthesia were randomly allocated to receive 0.75 μg/kg of dexmedetomidine (Dex group, n = 20), 0.15 mg/kg of nalbuphine (Nal group, n = 20), or a placebo (control group, n = 20) intravenously over 10 min. At the same time, all study subjects received nebulized lidocaine for 15 min. The primary outcome was patient tolerance as assessed by a 5-point ADL comfort score, while secondary outcomes included satisfaction, coughing, pain, nausea and vital signs.</p><p><strong>Results: </strong>Patients undergoing ADL in the Nal group had higher tolerance scores than those in the control and Dex groups [4 (3,4) vs. 3 (2,2.75), P < 0.017, and 4 (3,4) vs. 2 (2,2,75), P < 0.001, respectively] and higher satisfaction [7 (6,8) vs. 4 (3,5.75), P < 0.017, and 7 (6,8) vs. 5.5 (5,6), P < 0.001, respectively]. Additionally, the Nal group had significantly fewer adverse events, such as pain and nausea than the control and Dex groups. The sedation score and peripheral oxygen and saturation were significantly higher in the Nal group than in the Dex group, with no difference between the Nal and control groups (P < 0.001, P = 0.159, respectively).</p><p><strong>Conclusions: </strong>Intravenous nalbuphine in combination with lidocaine aerosol inhalation significantly improved patient tolerance and satisfaction while reducing nausea, coughing, pain, sedation, and SpO<sub>2</sub> levels during ADL.</p>\",\"PeriodicalId\":19764,\"journal\":{\"name\":\"Perioperative Medicine\",\"volume\":\"13 1\",\"pages\":\"105\"},\"PeriodicalIF\":2.1000,\"publicationDate\":\"2024-10-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11490102/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Perioperative Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s13741-024-00461-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Perioperative Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s13741-024-00461-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Comparison of intravenous nalbuphine and dexmedetomidine in combination with lidocaine aerosol inhalation in awake direct laryngoscopy: a randomized, double-blind, placebo-controlled trial.
Background: The airway should be thoroughly and accurately evaluated before anesthesia induction and endotracheal intubation. Awake direct laryngoscopy (ADL) can provide rapid, accurate, and intuitive airway assessment, especially for suspected difficult airways, and sometimes eliminates the need for fiberoptic intubation in some suspicious difficult airway cases. However, an optimal regimen has not been determined.
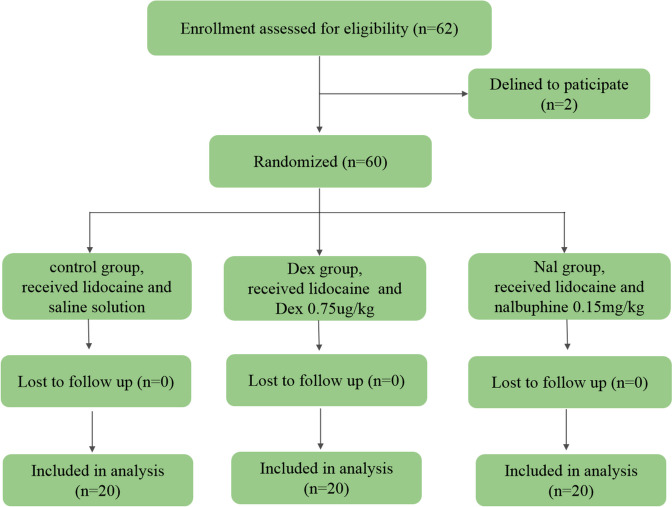
Methods: In this double-blind, controlled study, prior to ADL, 60 patients scheduled for general anesthesia were randomly allocated to receive 0.75 μg/kg of dexmedetomidine (Dex group, n = 20), 0.15 mg/kg of nalbuphine (Nal group, n = 20), or a placebo (control group, n = 20) intravenously over 10 min. At the same time, all study subjects received nebulized lidocaine for 15 min. The primary outcome was patient tolerance as assessed by a 5-point ADL comfort score, while secondary outcomes included satisfaction, coughing, pain, nausea and vital signs.
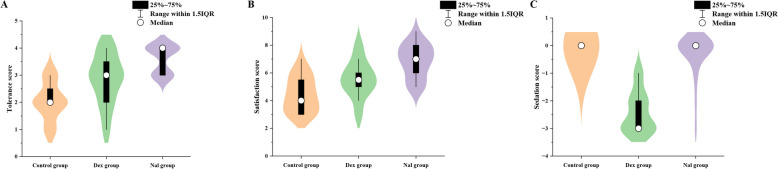
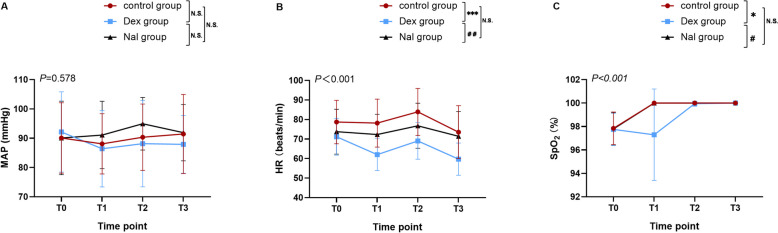
Results: Patients undergoing ADL in the Nal group had higher tolerance scores than those in the control and Dex groups [4 (3,4) vs. 3 (2,2.75), P < 0.017, and 4 (3,4) vs. 2 (2,2,75), P < 0.001, respectively] and higher satisfaction [7 (6,8) vs. 4 (3,5.75), P < 0.017, and 7 (6,8) vs. 5.5 (5,6), P < 0.001, respectively]. Additionally, the Nal group had significantly fewer adverse events, such as pain and nausea than the control and Dex groups. The sedation score and peripheral oxygen and saturation were significantly higher in the Nal group than in the Dex group, with no difference between the Nal and control groups (P < 0.001, P = 0.159, respectively).
Conclusions: Intravenous nalbuphine in combination with lidocaine aerosol inhalation significantly improved patient tolerance and satisfaction while reducing nausea, coughing, pain, sedation, and SpO2 levels during ADL.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


