Parsa Rouzrokh, Malihe Rezaee, Zahra Mohammadipour, Sasan Tavana, Isa Khaheshi, Ali Sheikhy, Taraneh Faghihi Langroudi
{"title":"放射学右心应变指数与 COVID-19 患者肺实质受累严重程度和预后的关系。","authors":"Parsa Rouzrokh, Malihe Rezaee, Zahra Mohammadipour, Sasan Tavana, Isa Khaheshi, Ali Sheikhy, Taraneh Faghihi Langroudi","doi":"10.34172/jcvtr.33094","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>It has been demonstrated that an increase in the diameter of the right ventricle or pulmonary artery in COVID-19 patients could be associated with the severity of lung involvement and may lead to unfavorable outcomes, particularly in the presence of pulmonary vascular diseases. This study investigated the relationship between these right heart strain features, the extent of lung involvement, and their prognostic values in patients without vascular comorbidities.</p><p><strong>Methods: </strong>This study selected 154 consecutive patients with positive chest computed tomography (CT) findings and no evidence of concurrent pulmonary disease. Clinical characteristics and adverse outcomes in in-hospital settings were collected retrospectively. Diameters of cardiac ventricles and arteries, along with lung opacification scores, were obtained using CT pulmonary angiography (CTPA) findings, and the association of these variables was evaluated.</p><p><strong>Results: </strong>An increase in pulmonary artery (PA) to ascending aorta (AO) diameter ratio and lung parenchymal damage were significantly and positively correlated (<i>P</i>=0.017), but increased right ventricle (RV) to left ventricle (LV) diameter ratio showed no association with the extent of chest opacification (<i>P</i>=0.098). Evaluating the prognostic ability of both ratios using logistic regression and receiver operating characteristic (ROC) analysis proved no significant class separation in regards to predicting adverse outcomes (PA/AO: OR:1.081, <i>P</i> Value:0.638, RV/LV: OR:1.098, <i>P</i> Value:0.344).</p><p><strong>Conclusion: </strong>In COVID-19 patients without vascular comorbidities, a higher PA/AO diameter ratio was significantly associated with increased lung involvement severity on CT imaging but not with adverse in-hospital outcomes. Conversely, an increased RV/LV ratio on CTPA did not correlate significantly with adverse outcomes or the severity of parenchymal lung damage.</p>","PeriodicalId":15207,"journal":{"name":"Journal of Cardiovascular and Thoracic Research","volume":"16 3","pages":"171-178"},"PeriodicalIF":0.7000,"publicationDate":"2024-01-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489638/pdf/","citationCount":"0","resultStr":"{\"title\":\"The association of radiologic right heart strain indices with the severity of pulmonary parenchymal involvement and prognosis in patients with COVID-19.\",\"authors\":\"Parsa Rouzrokh, Malihe Rezaee, Zahra Mohammadipour, Sasan Tavana, Isa Khaheshi, Ali Sheikhy, Taraneh Faghihi Langroudi\",\"doi\":\"10.34172/jcvtr.33094\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>It has been demonstrated that an increase in the diameter of the right ventricle or pulmonary artery in COVID-19 patients could be associated with the severity of lung involvement and may lead to unfavorable outcomes, particularly in the presence of pulmonary vascular diseases. This study investigated the relationship between these right heart strain features, the extent of lung involvement, and their prognostic values in patients without vascular comorbidities.</p><p><strong>Methods: </strong>This study selected 154 consecutive patients with positive chest computed tomography (CT) findings and no evidence of concurrent pulmonary disease. Clinical characteristics and adverse outcomes in in-hospital settings were collected retrospectively. Diameters of cardiac ventricles and arteries, along with lung opacification scores, were obtained using CT pulmonary angiography (CTPA) findings, and the association of these variables was evaluated.</p><p><strong>Results: </strong>An increase in pulmonary artery (PA) to ascending aorta (AO) diameter ratio and lung parenchymal damage were significantly and positively correlated (<i>P</i>=0.017), but increased right ventricle (RV) to left ventricle (LV) diameter ratio showed no association with the extent of chest opacification (<i>P</i>=0.098). Evaluating the prognostic ability of both ratios using logistic regression and receiver operating characteristic (ROC) analysis proved no significant class separation in regards to predicting adverse outcomes (PA/AO: OR:1.081, <i>P</i> Value:0.638, RV/LV: OR:1.098, <i>P</i> Value:0.344).</p><p><strong>Conclusion: </strong>In COVID-19 patients without vascular comorbidities, a higher PA/AO diameter ratio was significantly associated with increased lung involvement severity on CT imaging but not with adverse in-hospital outcomes. Conversely, an increased RV/LV ratio on CTPA did not correlate significantly with adverse outcomes or the severity of parenchymal lung damage.</p>\",\"PeriodicalId\":15207,\"journal\":{\"name\":\"Journal of Cardiovascular and Thoracic Research\",\"volume\":\"16 3\",\"pages\":\"171-178\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-01-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11489638/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Cardiovascular and Thoracic Research\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.34172/jcvtr.33094\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Cardiovascular and Thoracic Research","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.34172/jcvtr.33094","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/20 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
The association of radiologic right heart strain indices with the severity of pulmonary parenchymal involvement and prognosis in patients with COVID-19.
Introduction: It has been demonstrated that an increase in the diameter of the right ventricle or pulmonary artery in COVID-19 patients could be associated with the severity of lung involvement and may lead to unfavorable outcomes, particularly in the presence of pulmonary vascular diseases. This study investigated the relationship between these right heart strain features, the extent of lung involvement, and their prognostic values in patients without vascular comorbidities.
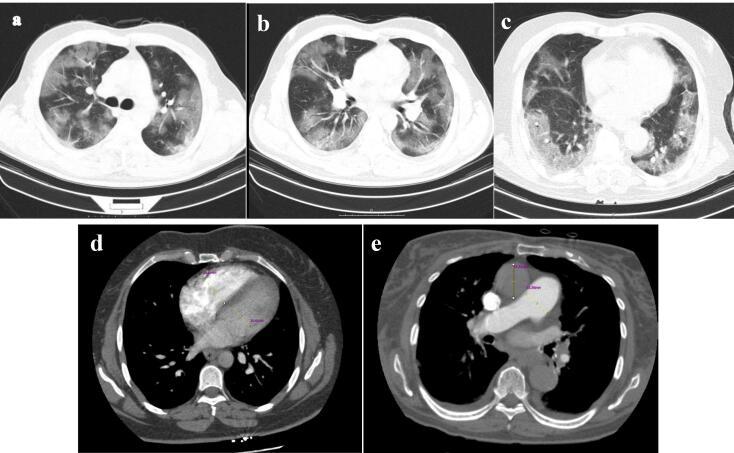
Methods: This study selected 154 consecutive patients with positive chest computed tomography (CT) findings and no evidence of concurrent pulmonary disease. Clinical characteristics and adverse outcomes in in-hospital settings were collected retrospectively. Diameters of cardiac ventricles and arteries, along with lung opacification scores, were obtained using CT pulmonary angiography (CTPA) findings, and the association of these variables was evaluated.
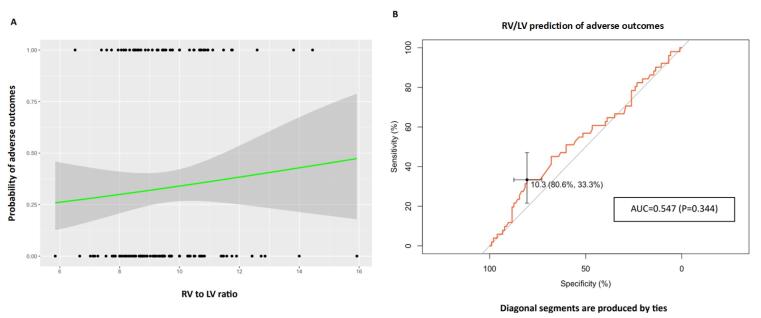
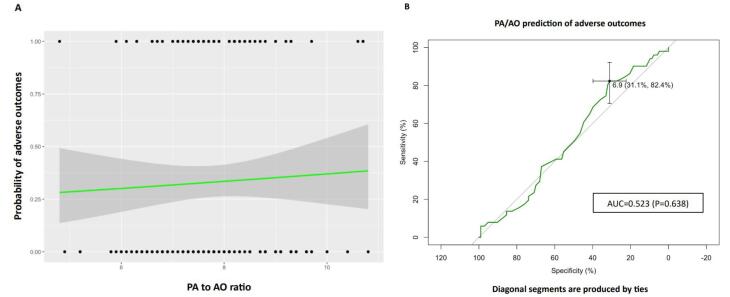
Results: An increase in pulmonary artery (PA) to ascending aorta (AO) diameter ratio and lung parenchymal damage were significantly and positively correlated (P=0.017), but increased right ventricle (RV) to left ventricle (LV) diameter ratio showed no association with the extent of chest opacification (P=0.098). Evaluating the prognostic ability of both ratios using logistic regression and receiver operating characteristic (ROC) analysis proved no significant class separation in regards to predicting adverse outcomes (PA/AO: OR:1.081, P Value:0.638, RV/LV: OR:1.098, P Value:0.344).
Conclusion: In COVID-19 patients without vascular comorbidities, a higher PA/AO diameter ratio was significantly associated with increased lung involvement severity on CT imaging but not with adverse in-hospital outcomes. Conversely, an increased RV/LV ratio on CTPA did not correlate significantly with adverse outcomes or the severity of parenchymal lung damage.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


