{"title":"高流量鼻腔气溶胶疗法;区域气溶胶沉积和气道反应性。","authors":"Srinivasa Potla, Gerald C Smaldone","doi":"10.1089/jamp.2024.0026","DOIUrl":null,"url":null,"abstract":"<p><p><b><i>Introduction:</i></b> In normal subjects, during tidal breathing, aerosols deposit by settling in small airways. With obstructive lung disease (OLD), collapse of airways during expiration causes turbulence and increased deposition in central airways. High-flow nasal cannula (HFNC) therapy, washing out dead space, may affect deposition mechanisms and drug delivery. This study compared aerosol deposition and airway responsiveness in OLD after traditional and HFNC nebulization therapy. <b><i>Methods:</i></b> Twelve subjects with moderate to severe OLD participated in a two-day study. Spirometry was measured pre- and post-aerosol inhalation. On Day 1 (D1) subjects tidally inhaled radiolabeled albuterol (<sup>99m</sup>Tc DTPA) by mouth via AeroTech II, (Biodex. Shirley, NY). Day 2 (D2) inhalation was via HFNC using <i>i-AIRE</i> (InspiRx, Inc. Somerset, NJ). The HFNC system (60 L/m) was infused by syringe pump at 50 mL/h. D2 lung deposition was monitored in real time by gamma camera to match D1. Pre and post heart rate, O<sub>2</sub> sat, and nasopharyngeal deposition (NP) were measured. Mechanistic contributions were modeled using multiple linear regression (MLR) of deposition rate (DR µg/m) as a function of breathing frequency, airway geometry (FEV<sub>1</sub>), and parenchymal integrity (DLCO). <b><i>Results:</i></b> Albuterol lung depositions were matched (<i>p</i> = 0.13) with D1 central/peripheral (sC/P) ratios 1.99 ± 0.98. Following HFNC, peripheral deposition increased (31% ± 33%, sC/P = 1.51 ± 0.43, <i>p</i> = 0.01). D2/D1% change FVC increased by 16.1 ± 16.7% (<i>p</i> = 0.003). NP deposition averaged 333% of lung. Heart rate and O<sub>2</sub> sat were unaffected (<i>p</i> = 0.31, <i>p</i> = 0.63 respectively). DR analysis was markedly different between D1 (<i>R</i><sup>2</sup> = 0.82) and D2 (<i>R</i><sup>2</sup> = 0.12). <b><i>Conclusion:</i></b> In subjects with OLD, HFNC nebulization at 60 L/min was well tolerated and increased peripheral drug delivery. Spirometry significantly improved. Systemic effects were undetected indicating limited nasal absorption. MLR demonstrated that different mechanisms of deposition govern traditional vs HFNC aerosol delivery. Breath-enhanced nebulization via HFNC may provide controllable and effective aerosol therapy in OLD.</p>","PeriodicalId":14940,"journal":{"name":"Journal of Aerosol Medicine and Pulmonary Drug Delivery","volume":" ","pages":"338-345"},"PeriodicalIF":1.8000,"publicationDate":"2024-12-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11669759/pdf/","citationCount":"0","resultStr":"{\"title\":\"High-Flow Nasal Aerosol Therapy; Regional Aerosol Deposition and Airway Responsiveness.\",\"authors\":\"Srinivasa Potla, Gerald C Smaldone\",\"doi\":\"10.1089/jamp.2024.0026\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p><b><i>Introduction:</i></b> In normal subjects, during tidal breathing, aerosols deposit by settling in small airways. With obstructive lung disease (OLD), collapse of airways during expiration causes turbulence and increased deposition in central airways. High-flow nasal cannula (HFNC) therapy, washing out dead space, may affect deposition mechanisms and drug delivery. This study compared aerosol deposition and airway responsiveness in OLD after traditional and HFNC nebulization therapy. <b><i>Methods:</i></b> Twelve subjects with moderate to severe OLD participated in a two-day study. Spirometry was measured pre- and post-aerosol inhalation. On Day 1 (D1) subjects tidally inhaled radiolabeled albuterol (<sup>99m</sup>Tc DTPA) by mouth via AeroTech II, (Biodex. Shirley, NY). Day 2 (D2) inhalation was via HFNC using <i>i-AIRE</i> (InspiRx, Inc. Somerset, NJ). The HFNC system (60 L/m) was infused by syringe pump at 50 mL/h. D2 lung deposition was monitored in real time by gamma camera to match D1. Pre and post heart rate, O<sub>2</sub> sat, and nasopharyngeal deposition (NP) were measured. Mechanistic contributions were modeled using multiple linear regression (MLR) of deposition rate (DR µg/m) as a function of breathing frequency, airway geometry (FEV<sub>1</sub>), and parenchymal integrity (DLCO). <b><i>Results:</i></b> Albuterol lung depositions were matched (<i>p</i> = 0.13) with D1 central/peripheral (sC/P) ratios 1.99 ± 0.98. Following HFNC, peripheral deposition increased (31% ± 33%, sC/P = 1.51 ± 0.43, <i>p</i> = 0.01). D2/D1% change FVC increased by 16.1 ± 16.7% (<i>p</i> = 0.003). NP deposition averaged 333% of lung. Heart rate and O<sub>2</sub> sat were unaffected (<i>p</i> = 0.31, <i>p</i> = 0.63 respectively). DR analysis was markedly different between D1 (<i>R</i><sup>2</sup> = 0.82) and D2 (<i>R</i><sup>2</sup> = 0.12). <b><i>Conclusion:</i></b> In subjects with OLD, HFNC nebulization at 60 L/min was well tolerated and increased peripheral drug delivery. Spirometry significantly improved. Systemic effects were undetected indicating limited nasal absorption. MLR demonstrated that different mechanisms of deposition govern traditional vs HFNC aerosol delivery. Breath-enhanced nebulization via HFNC may provide controllable and effective aerosol therapy in OLD.</p>\",\"PeriodicalId\":14940,\"journal\":{\"name\":\"Journal of Aerosol Medicine and Pulmonary Drug Delivery\",\"volume\":\" \",\"pages\":\"338-345\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-12-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11669759/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Journal of Aerosol Medicine and Pulmonary Drug Delivery\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1089/jamp.2024.0026\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/22 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q3\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Journal of Aerosol Medicine and Pulmonary Drug Delivery","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1089/jamp.2024.0026","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/22 0:00:00","PubModel":"Epub","JCR":"Q3","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
High-Flow Nasal Aerosol Therapy; Regional Aerosol Deposition and Airway Responsiveness.
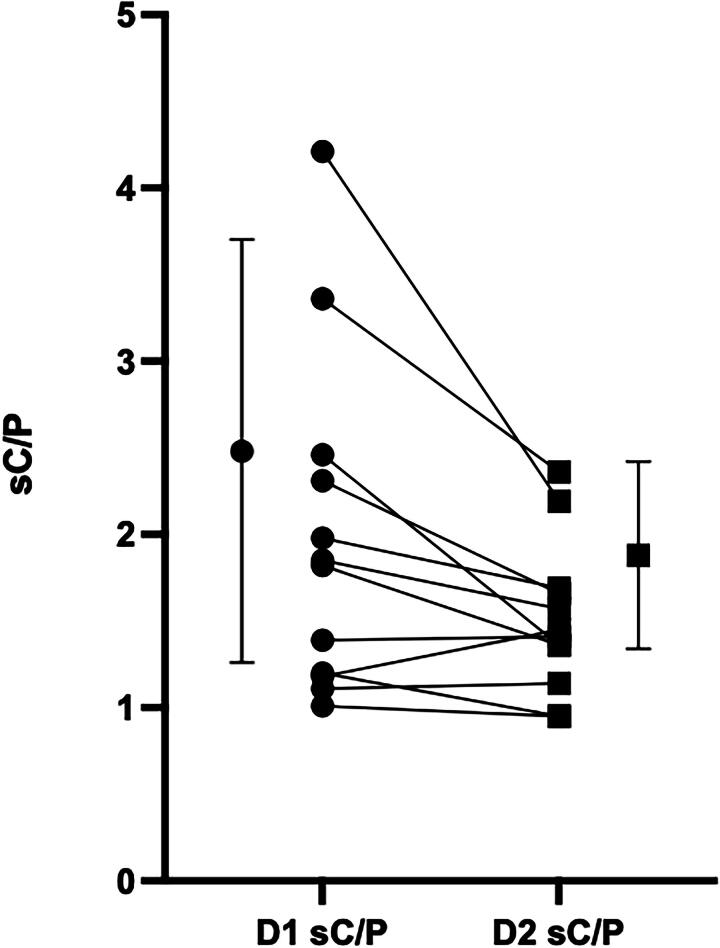
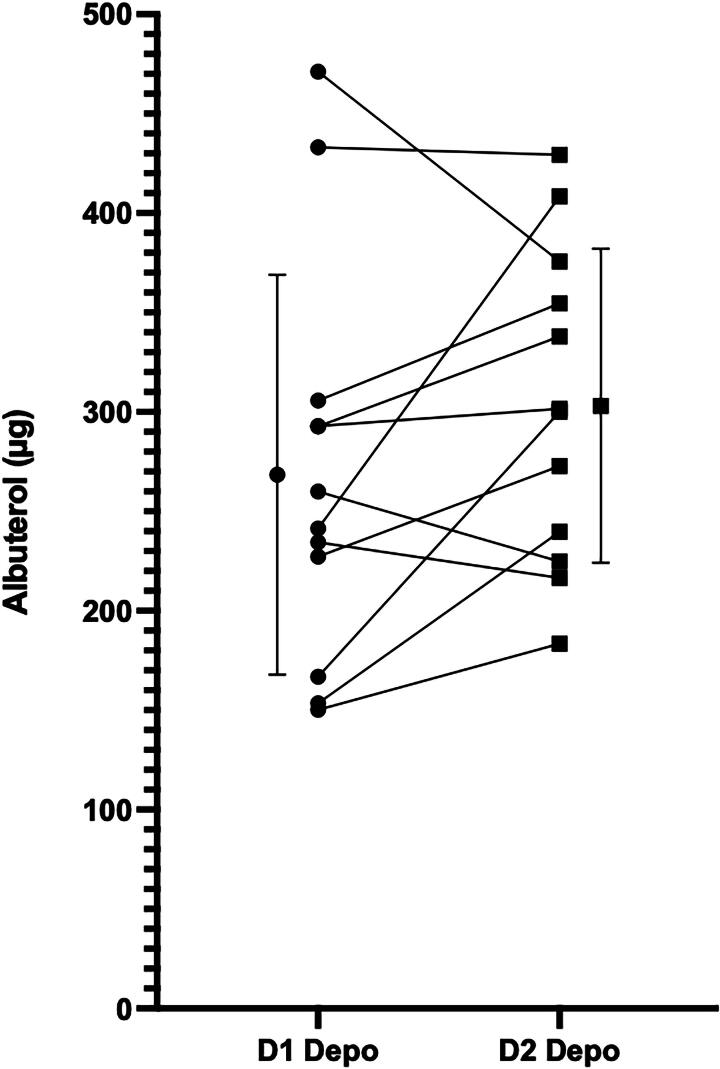
Introduction: In normal subjects, during tidal breathing, aerosols deposit by settling in small airways. With obstructive lung disease (OLD), collapse of airways during expiration causes turbulence and increased deposition in central airways. High-flow nasal cannula (HFNC) therapy, washing out dead space, may affect deposition mechanisms and drug delivery. This study compared aerosol deposition and airway responsiveness in OLD after traditional and HFNC nebulization therapy. Methods: Twelve subjects with moderate to severe OLD participated in a two-day study. Spirometry was measured pre- and post-aerosol inhalation. On Day 1 (D1) subjects tidally inhaled radiolabeled albuterol (99mTc DTPA) by mouth via AeroTech II, (Biodex. Shirley, NY). Day 2 (D2) inhalation was via HFNC using i-AIRE (InspiRx, Inc. Somerset, NJ). The HFNC system (60 L/m) was infused by syringe pump at 50 mL/h. D2 lung deposition was monitored in real time by gamma camera to match D1. Pre and post heart rate, O2 sat, and nasopharyngeal deposition (NP) were measured. Mechanistic contributions were modeled using multiple linear regression (MLR) of deposition rate (DR µg/m) as a function of breathing frequency, airway geometry (FEV1), and parenchymal integrity (DLCO). Results: Albuterol lung depositions were matched (p = 0.13) with D1 central/peripheral (sC/P) ratios 1.99 ± 0.98. Following HFNC, peripheral deposition increased (31% ± 33%, sC/P = 1.51 ± 0.43, p = 0.01). D2/D1% change FVC increased by 16.1 ± 16.7% (p = 0.003). NP deposition averaged 333% of lung. Heart rate and O2 sat were unaffected (p = 0.31, p = 0.63 respectively). DR analysis was markedly different between D1 (R2 = 0.82) and D2 (R2 = 0.12). Conclusion: In subjects with OLD, HFNC nebulization at 60 L/min was well tolerated and increased peripheral drug delivery. Spirometry significantly improved. Systemic effects were undetected indicating limited nasal absorption. MLR demonstrated that different mechanisms of deposition govern traditional vs HFNC aerosol delivery. Breath-enhanced nebulization via HFNC may provide controllable and effective aerosol therapy in OLD.
期刊介绍:
Journal of Aerosol Medicine and Pulmonary Drug Delivery is the only peer-reviewed journal delivering innovative, authoritative coverage of the health effects of inhaled aerosols and delivery of drugs through the pulmonary system. The Journal is a forum for leading experts, addressing novel topics such as aerosolized chemotherapy, aerosolized vaccines, methods to determine toxicities, and delivery of aerosolized drugs in the intubated patient.
Journal of Aerosol Medicine and Pulmonary Drug Delivery coverage includes:
Pulmonary drug delivery
Airway reactivity and asthma treatment
Inhalation of particles and gases in the respiratory tract
Toxic effects of inhaled agents
Aerosols as tools for studying basic physiologic phenomena.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


