Angela J Forbes, Chris M A Frampton, Andrew S Day, Millie DeVries, Nina McVicar, Heidi Su, Richard B Gearry
{"title":"新西兰坎特伯雷炎症性肠病患者前瞻性人群发病队列的十年结果","authors":"Angela J Forbes, Chris M A Frampton, Andrew S Day, Millie DeVries, Nina McVicar, Heidi Su, Richard B Gearry","doi":"10.1002/jgh3.70038","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background and Aim</h3>\n \n <p>Inflammatory bowel disease (IBD) is a progressive condition where ongoing inflammation in the gastrointestinal tract can lead to complications such as strictures, and fistulae. The long-term outcomes of newly diagnosed patients under current medical therapy can be used to plan health service provision and guide patients.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>Prospective population-based data on all incident patients diagnosed with IBD in Canterbury was gathered in 2014 (<i>n</i> = 205). The medical records of these patients were followed for medication use, disease progression, hospitalization, surgery and mortality, in the 10 years since their diagnosis. Survival analysis and cox regression determined characteristics associated with earlier time to these outcomes.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Medical records of 184 IBD patients were able to be retrieved. Immunomodulators were used by 62% and biologics by 35%; hospitalization occurred for 42% and surgery for 15%. Montreal phenotype progression occurred for 21 and 7% of the cohort died. Younger age at diagnosis hazard ratio (HR) 2.1 (95% confidence interval [CI] 1.1–4.0) and Crohn's disease HR 1.7 (95% CI 1.1–2.6) was associated with immunomodulator use. Younger age was also associated with biologic use HR 2.9 (95% CI 1.2–6.9). Male gender was associated with surgery HR 2.8 (95% CI 1.2–6.4). Perianal disease at diagnosis (14.7%) was associated with immunomodulator use HR 2.58 (95% CI 1.44–4.59) and Montreal phenotype progression HR 2.93 (95% CI 1.10–7.77).</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>In the 10 years since diagnosis disease progression and treatment escalation occurred for most of this population-based cohort. Earlier intervention for patients with higher-risk characteristics may improve long-term outcomes reducing the burden on health systems.</p>\n </section>\n </div>","PeriodicalId":45861,"journal":{"name":"JGH Open","volume":"8 10","pages":""},"PeriodicalIF":1.7000,"publicationDate":"2024-10-14","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.70038","citationCount":"0","resultStr":"{\"title\":\"Ten-year outcomes of a prospective population-based incidence cohort of inflammatory bowel disease patients from Canterbury, New Zealand\",\"authors\":\"Angela J Forbes, Chris M A Frampton, Andrew S Day, Millie DeVries, Nina McVicar, Heidi Su, Richard B Gearry\",\"doi\":\"10.1002/jgh3.70038\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background and Aim</h3>\\n \\n <p>Inflammatory bowel disease (IBD) is a progressive condition where ongoing inflammation in the gastrointestinal tract can lead to complications such as strictures, and fistulae. The long-term outcomes of newly diagnosed patients under current medical therapy can be used to plan health service provision and guide patients.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>Prospective population-based data on all incident patients diagnosed with IBD in Canterbury was gathered in 2014 (<i>n</i> = 205). The medical records of these patients were followed for medication use, disease progression, hospitalization, surgery and mortality, in the 10 years since their diagnosis. Survival analysis and cox regression determined characteristics associated with earlier time to these outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Medical records of 184 IBD patients were able to be retrieved. Immunomodulators were used by 62% and biologics by 35%; hospitalization occurred for 42% and surgery for 15%. Montreal phenotype progression occurred for 21 and 7% of the cohort died. Younger age at diagnosis hazard ratio (HR) 2.1 (95% confidence interval [CI] 1.1–4.0) and Crohn's disease HR 1.7 (95% CI 1.1–2.6) was associated with immunomodulator use. Younger age was also associated with biologic use HR 2.9 (95% CI 1.2–6.9). Male gender was associated with surgery HR 2.8 (95% CI 1.2–6.4). Perianal disease at diagnosis (14.7%) was associated with immunomodulator use HR 2.58 (95% CI 1.44–4.59) and Montreal phenotype progression HR 2.93 (95% CI 1.10–7.77).</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>In the 10 years since diagnosis disease progression and treatment escalation occurred for most of this population-based cohort. Earlier intervention for patients with higher-risk characteristics may improve long-term outcomes reducing the burden on health systems.</p>\\n </section>\\n </div>\",\"PeriodicalId\":45861,\"journal\":{\"name\":\"JGH Open\",\"volume\":\"8 10\",\"pages\":\"\"},\"PeriodicalIF\":1.7000,\"publicationDate\":\"2024-10-14\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1002/jgh3.70038\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"JGH Open\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70038\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"JGH Open","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/jgh3.70038","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Ten-year outcomes of a prospective population-based incidence cohort of inflammatory bowel disease patients from Canterbury, New Zealand
Background and Aim
Inflammatory bowel disease (IBD) is a progressive condition where ongoing inflammation in the gastrointestinal tract can lead to complications such as strictures, and fistulae. The long-term outcomes of newly diagnosed patients under current medical therapy can be used to plan health service provision and guide patients.
Methods
Prospective population-based data on all incident patients diagnosed with IBD in Canterbury was gathered in 2014 (n = 205). The medical records of these patients were followed for medication use, disease progression, hospitalization, surgery and mortality, in the 10 years since their diagnosis. Survival analysis and cox regression determined characteristics associated with earlier time to these outcomes.
Results
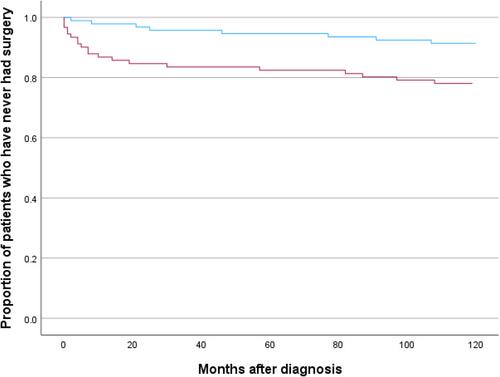
Medical records of 184 IBD patients were able to be retrieved. Immunomodulators were used by 62% and biologics by 35%; hospitalization occurred for 42% and surgery for 15%. Montreal phenotype progression occurred for 21 and 7% of the cohort died. Younger age at diagnosis hazard ratio (HR) 2.1 (95% confidence interval [CI] 1.1–4.0) and Crohn's disease HR 1.7 (95% CI 1.1–2.6) was associated with immunomodulator use. Younger age was also associated with biologic use HR 2.9 (95% CI 1.2–6.9). Male gender was associated with surgery HR 2.8 (95% CI 1.2–6.4). Perianal disease at diagnosis (14.7%) was associated with immunomodulator use HR 2.58 (95% CI 1.44–4.59) and Montreal phenotype progression HR 2.93 (95% CI 1.10–7.77).
Conclusion
In the 10 years since diagnosis disease progression and treatment escalation occurred for most of this population-based cohort. Earlier intervention for patients with higher-risk characteristics may improve long-term outcomes reducing the burden on health systems.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


