Hervé Monka Lekuya, Jelle Vandersteene, Larrey Kasereka Kamabu, Rose Nantambi, Ronald Mbiine, Anthony Kirabira, Fredrick Makumbi, Stephen Cose, David Patrick Kateete, Mark Kaddumukasa, Edward Baert, Moses Galukande, Jean-Pierre Okito Kalala
{"title":"撒哈拉以南地区一家三级医院中凹陷性颅骨骨折患者的手术时机和手术部位感染的术前预测因素:前瞻性队列研究","authors":"Hervé Monka Lekuya, Jelle Vandersteene, Larrey Kasereka Kamabu, Rose Nantambi, Ronald Mbiine, Anthony Kirabira, Fredrick Makumbi, Stephen Cose, David Patrick Kateete, Mark Kaddumukasa, Edward Baert, Moses Galukande, Jean-Pierre Okito Kalala","doi":"10.1089/neur.2024.0088","DOIUrl":null,"url":null,"abstract":"<p><p>Surgical site infections (SSIs) remain a major cause of life-threatening morbidity following surgery for depressed skull fractures (DSFs) among patients with traumatic brain injury (TBI). The timing of the surgery for DSF has been questioned as a risk of SSI without a clear cutoff. We aimed to compare the risk of SSI within 3 months between surgery done before versus after 48 h of injury and with its preoperative predictors. We conducted a prospective cohort study at Mulago Hospital, Uganda. Patients with mild-to-moderate TBI with DSF were followed up perioperatively from the operating time up to 3 months. The outcome variables were the incidence risk of SSI, types of SSI, microbial culture patterns of wound isolates, and hospital length of stay. We enrolled 127 patients with DSF, median age = 24 (interquartile range [IQR] = 17-31 years), 88.2% (112/127) male, and assault victims = 53.5%. The frontal bone involved 59%, while 50.4% had a dural tear. The incidence of SSI was 18.9%, mainly superficial incisional infection; Gram-negative microorganisms were the most common isolates (64.7%). The group of surgical intervention >48 h had an increased incidence of SSI (57.3% vs. 42.7%, <i>p</i> = 0.006), a longer median of postoperative hospital stay (8[IQR = 6-12] days versus 5 [IQR = 4-9], [<i>p</i> < 0.001]), and a higher rate of reoperation (71.4% vs. 28.6%, <i>p</i> = 0.05) in comparison with the group of ≤48 h. In multivariate analysis between the group of SSI and no SSI, surgical timing >48 h (95% confidence interval [CI], 1.25-6.22), pneumocranium on computed tomography [CT] scan (95% CI: 1.50-5.36), and involvement of air sinus (95% CI: 1.55-5.47) were associated with a >2.5-fold increase in the rate of SSI. The SSI group had a longer median hospital stay (<i>p</i> value <0.001). The SSI risk in DSF is high following a surgical intervention >48 h of injury, with predictors such as the frontal location of DSF, pneumocranium on a CT scan, and involvement of the air sinus. We recommend early surgical intervention within 48 h of injury.</p>","PeriodicalId":74300,"journal":{"name":"Neurotrauma reports","volume":"5 1","pages":"824-844"},"PeriodicalIF":1.8000,"publicationDate":"2024-09-20","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11462418/pdf/","citationCount":"0","resultStr":"{\"title\":\"Timing of Surgery and Preoperative Predictors of Surgical Site Infections for Patients with Depressed Skull Fractures in a Sub-Saharan Tertiary Hospital: A Prospective Cohort Study.\",\"authors\":\"Hervé Monka Lekuya, Jelle Vandersteene, Larrey Kasereka Kamabu, Rose Nantambi, Ronald Mbiine, Anthony Kirabira, Fredrick Makumbi, Stephen Cose, David Patrick Kateete, Mark Kaddumukasa, Edward Baert, Moses Galukande, Jean-Pierre Okito Kalala\",\"doi\":\"10.1089/neur.2024.0088\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Surgical site infections (SSIs) remain a major cause of life-threatening morbidity following surgery for depressed skull fractures (DSFs) among patients with traumatic brain injury (TBI). The timing of the surgery for DSF has been questioned as a risk of SSI without a clear cutoff. We aimed to compare the risk of SSI within 3 months between surgery done before versus after 48 h of injury and with its preoperative predictors. We conducted a prospective cohort study at Mulago Hospital, Uganda. Patients with mild-to-moderate TBI with DSF were followed up perioperatively from the operating time up to 3 months. The outcome variables were the incidence risk of SSI, types of SSI, microbial culture patterns of wound isolates, and hospital length of stay. We enrolled 127 patients with DSF, median age = 24 (interquartile range [IQR] = 17-31 years), 88.2% (112/127) male, and assault victims = 53.5%. The frontal bone involved 59%, while 50.4% had a dural tear. The incidence of SSI was 18.9%, mainly superficial incisional infection; Gram-negative microorganisms were the most common isolates (64.7%). The group of surgical intervention >48 h had an increased incidence of SSI (57.3% vs. 42.7%, <i>p</i> = 0.006), a longer median of postoperative hospital stay (8[IQR = 6-12] days versus 5 [IQR = 4-9], [<i>p</i> < 0.001]), and a higher rate of reoperation (71.4% vs. 28.6%, <i>p</i> = 0.05) in comparison with the group of ≤48 h. In multivariate analysis between the group of SSI and no SSI, surgical timing >48 h (95% confidence interval [CI], 1.25-6.22), pneumocranium on computed tomography [CT] scan (95% CI: 1.50-5.36), and involvement of air sinus (95% CI: 1.55-5.47) were associated with a >2.5-fold increase in the rate of SSI. The SSI group had a longer median hospital stay (<i>p</i> value <0.001). The SSI risk in DSF is high following a surgical intervention >48 h of injury, with predictors such as the frontal location of DSF, pneumocranium on a CT scan, and involvement of the air sinus. We recommend early surgical intervention within 48 h of injury.</p>\",\"PeriodicalId\":74300,\"journal\":{\"name\":\"Neurotrauma reports\",\"volume\":\"5 1\",\"pages\":\"824-844\"},\"PeriodicalIF\":1.8000,\"publicationDate\":\"2024-09-20\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11462418/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Neurotrauma reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1089/neur.2024.0088\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"CLINICAL NEUROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Neurotrauma reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1089/neur.2024.0088","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"CLINICAL NEUROLOGY","Score":null,"Total":0}
Timing of Surgery and Preoperative Predictors of Surgical Site Infections for Patients with Depressed Skull Fractures in a Sub-Saharan Tertiary Hospital: A Prospective Cohort Study.
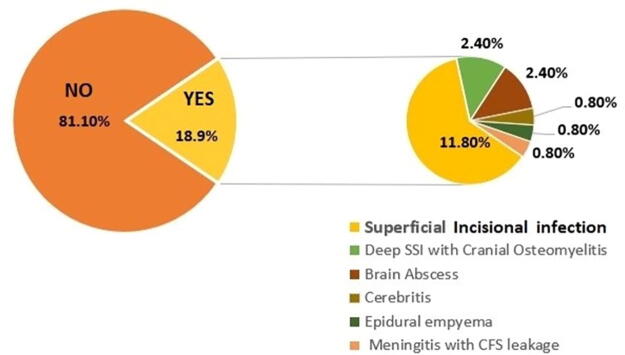
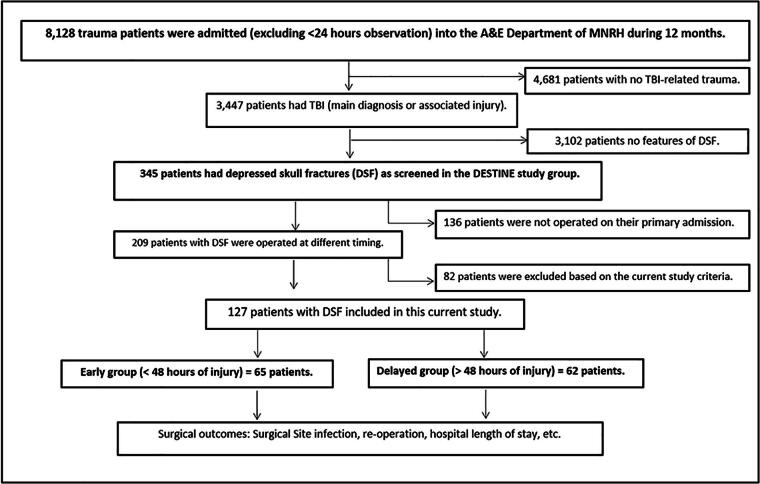
Surgical site infections (SSIs) remain a major cause of life-threatening morbidity following surgery for depressed skull fractures (DSFs) among patients with traumatic brain injury (TBI). The timing of the surgery for DSF has been questioned as a risk of SSI without a clear cutoff. We aimed to compare the risk of SSI within 3 months between surgery done before versus after 48 h of injury and with its preoperative predictors. We conducted a prospective cohort study at Mulago Hospital, Uganda. Patients with mild-to-moderate TBI with DSF were followed up perioperatively from the operating time up to 3 months. The outcome variables were the incidence risk of SSI, types of SSI, microbial culture patterns of wound isolates, and hospital length of stay. We enrolled 127 patients with DSF, median age = 24 (interquartile range [IQR] = 17-31 years), 88.2% (112/127) male, and assault victims = 53.5%. The frontal bone involved 59%, while 50.4% had a dural tear. The incidence of SSI was 18.9%, mainly superficial incisional infection; Gram-negative microorganisms were the most common isolates (64.7%). The group of surgical intervention >48 h had an increased incidence of SSI (57.3% vs. 42.7%, p = 0.006), a longer median of postoperative hospital stay (8[IQR = 6-12] days versus 5 [IQR = 4-9], [p < 0.001]), and a higher rate of reoperation (71.4% vs. 28.6%, p = 0.05) in comparison with the group of ≤48 h. In multivariate analysis between the group of SSI and no SSI, surgical timing >48 h (95% confidence interval [CI], 1.25-6.22), pneumocranium on computed tomography [CT] scan (95% CI: 1.50-5.36), and involvement of air sinus (95% CI: 1.55-5.47) were associated with a >2.5-fold increase in the rate of SSI. The SSI group had a longer median hospital stay (p value <0.001). The SSI risk in DSF is high following a surgical intervention >48 h of injury, with predictors such as the frontal location of DSF, pneumocranium on a CT scan, and involvement of the air sinus. We recommend early surgical intervention within 48 h of injury.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


