Lukas Juergensen, Robert Rischen, Max Toennemann, Georg Gosheger, Dominic Gehweiler, Martin Schulze
{"title":"用于 3d 打印的骨盆骨分割的准确性:基于解剖地标的分割准确性研究,以评估观察者的影响。","authors":"Lukas Juergensen, Robert Rischen, Max Toennemann, Georg Gosheger, Dominic Gehweiler, Martin Schulze","doi":"10.1186/s41205-024-00237-8","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>3D printing has a wide range of applications and has brought significant change to many medical fields. However, ensuring quality assurance (QA) is essential for patient safety and requires a QA program that encompasses the entire production process. This process begins with imaging and continues on with segmentation, which is the conversion of Digital Imaging and Communications in Medicine (DICOM) data into virtual 3D-models. Since segmentation is highly influenced by manual intervention the influence of the users background on segmentation accuracy should be thoroughly investigated.</p><p><strong>Methods: </strong>Seventeen computed tomography (CT) scans of the pelvis with physiological bony structures were identified, anonymized, exported as DICOM data sets, and pelvic bones were segmented by four observers with different backgrounds. Landmarks were measured on DICOM images and in the segmentations. Intraclass correlation coefficients (ICCs) were calculated to assess inter-observer agreement, and the trueness of the segmentation results was analyzed by comparing the DICOM landmark measurements with the measurements of the segmentation results. The correlation between segmentation trueness and segmentation time was analyzed.</p><p><strong>Results: </strong>The lower limits of the 95% confidence intervals of the ICCs for the seven landmarks analyzed ranged from 0.511 to 0.986. The distance between the iliac crests showed the highest agreement between observers, while the distance between the ischial tuberosities showed the lowest. The distance between the upper edge of the symphysis and the promontory showed the lowest deviation between DICOM measurements and segmentation measurements (mean deviations < 1 mm), while the intertuberous distance showed the highest deviation (mean deviations 14.5-18.2 mm).</p><p><strong>Conclusions: </strong>Investigators with diverse backgrounds in segmentation and varying experience with slice images achieved pelvic bone segmentations with landmark measurements of mostly high agreement in a setup with high realism. In contrast, high variability was observed in the segmentation of the coccyx. In general, interobserver agreement was high, but due to measurement inaccuracies, landmark-based approaches cannot conclusively show that segmentation accuracy is within a clinically tolerable range of 2 mm for the pelvis. If the segmentation is performed by a very inexperienced user, the result should be reviewed critically by the clinician in charge.</p>","PeriodicalId":72036,"journal":{"name":"3D printing in medicine","volume":"10 1","pages":"33"},"PeriodicalIF":3.1000,"publicationDate":"2024-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11460233/pdf/","citationCount":"0","resultStr":"{\"title\":\"Accuracy of pelvic bone segmentation for 3d printing: a study of segmentation accuracy based on anatomic landmarks to evaluate the influence of the observer.\",\"authors\":\"Lukas Juergensen, Robert Rischen, Max Toennemann, Georg Gosheger, Dominic Gehweiler, Martin Schulze\",\"doi\":\"10.1186/s41205-024-00237-8\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>3D printing has a wide range of applications and has brought significant change to many medical fields. However, ensuring quality assurance (QA) is essential for patient safety and requires a QA program that encompasses the entire production process. This process begins with imaging and continues on with segmentation, which is the conversion of Digital Imaging and Communications in Medicine (DICOM) data into virtual 3D-models. Since segmentation is highly influenced by manual intervention the influence of the users background on segmentation accuracy should be thoroughly investigated.</p><p><strong>Methods: </strong>Seventeen computed tomography (CT) scans of the pelvis with physiological bony structures were identified, anonymized, exported as DICOM data sets, and pelvic bones were segmented by four observers with different backgrounds. Landmarks were measured on DICOM images and in the segmentations. Intraclass correlation coefficients (ICCs) were calculated to assess inter-observer agreement, and the trueness of the segmentation results was analyzed by comparing the DICOM landmark measurements with the measurements of the segmentation results. The correlation between segmentation trueness and segmentation time was analyzed.</p><p><strong>Results: </strong>The lower limits of the 95% confidence intervals of the ICCs for the seven landmarks analyzed ranged from 0.511 to 0.986. The distance between the iliac crests showed the highest agreement between observers, while the distance between the ischial tuberosities showed the lowest. The distance between the upper edge of the symphysis and the promontory showed the lowest deviation between DICOM measurements and segmentation measurements (mean deviations < 1 mm), while the intertuberous distance showed the highest deviation (mean deviations 14.5-18.2 mm).</p><p><strong>Conclusions: </strong>Investigators with diverse backgrounds in segmentation and varying experience with slice images achieved pelvic bone segmentations with landmark measurements of mostly high agreement in a setup with high realism. In contrast, high variability was observed in the segmentation of the coccyx. In general, interobserver agreement was high, but due to measurement inaccuracies, landmark-based approaches cannot conclusively show that segmentation accuracy is within a clinically tolerable range of 2 mm for the pelvis. If the segmentation is performed by a very inexperienced user, the result should be reviewed critically by the clinician in charge.</p>\",\"PeriodicalId\":72036,\"journal\":{\"name\":\"3D printing in medicine\",\"volume\":\"10 1\",\"pages\":\"33\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-10-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11460233/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"3D printing in medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1186/s41205-024-00237-8\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"3D printing in medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1186/s41205-024-00237-8","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"RADIOLOGY, NUCLEAR MEDICINE & MEDICAL IMAGING","Score":null,"Total":0}
Accuracy of pelvic bone segmentation for 3d printing: a study of segmentation accuracy based on anatomic landmarks to evaluate the influence of the observer.
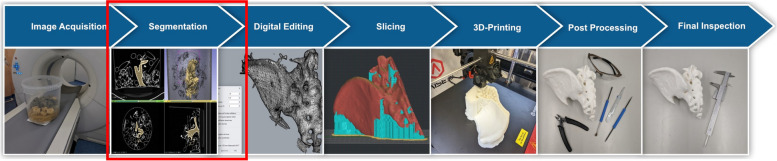
Background: 3D printing has a wide range of applications and has brought significant change to many medical fields. However, ensuring quality assurance (QA) is essential for patient safety and requires a QA program that encompasses the entire production process. This process begins with imaging and continues on with segmentation, which is the conversion of Digital Imaging and Communications in Medicine (DICOM) data into virtual 3D-models. Since segmentation is highly influenced by manual intervention the influence of the users background on segmentation accuracy should be thoroughly investigated.
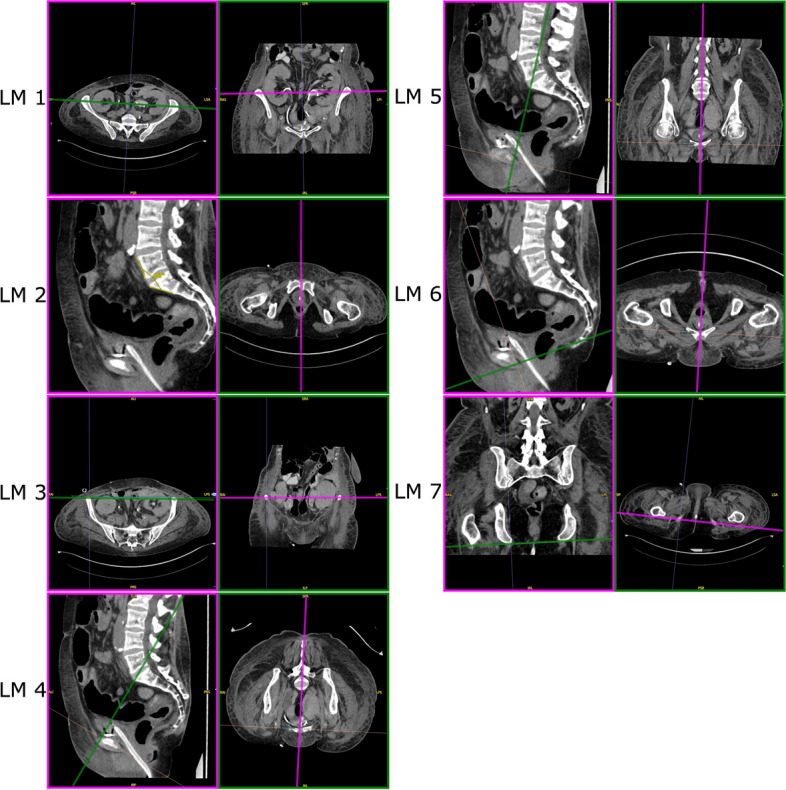
Methods: Seventeen computed tomography (CT) scans of the pelvis with physiological bony structures were identified, anonymized, exported as DICOM data sets, and pelvic bones were segmented by four observers with different backgrounds. Landmarks were measured on DICOM images and in the segmentations. Intraclass correlation coefficients (ICCs) were calculated to assess inter-observer agreement, and the trueness of the segmentation results was analyzed by comparing the DICOM landmark measurements with the measurements of the segmentation results. The correlation between segmentation trueness and segmentation time was analyzed.
Results: The lower limits of the 95% confidence intervals of the ICCs for the seven landmarks analyzed ranged from 0.511 to 0.986. The distance between the iliac crests showed the highest agreement between observers, while the distance between the ischial tuberosities showed the lowest. The distance between the upper edge of the symphysis and the promontory showed the lowest deviation between DICOM measurements and segmentation measurements (mean deviations < 1 mm), while the intertuberous distance showed the highest deviation (mean deviations 14.5-18.2 mm).
Conclusions: Investigators with diverse backgrounds in segmentation and varying experience with slice images achieved pelvic bone segmentations with landmark measurements of mostly high agreement in a setup with high realism. In contrast, high variability was observed in the segmentation of the coccyx. In general, interobserver agreement was high, but due to measurement inaccuracies, landmark-based approaches cannot conclusively show that segmentation accuracy is within a clinically tolerable range of 2 mm for the pelvis. If the segmentation is performed by a very inexperienced user, the result should be reviewed critically by the clinician in charge.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


