{"title":"视频辅助胸腔镜手术前在 CT 引导下进行肺结节微线圈定位与钩丝定位的比较,无需透视引导。","authors":"Xuedong Sun, Jinxin Fu, Chao Ma, Zhenfei Song, Siwei Yang, Long Jin, Feng Duan","doi":"10.1186/s12890-024-03306-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Both microcoils and hook-wires are commonly utilized for preoperative pulmonary nodule localization due to their convenience, but it remains unclear which one should be prioritized for recommendation.</p><p><strong>Aims: </strong>To compare the safety and efficacy of microcoils and hook-wires for pulmonary nodule localization.</p><p><strong>Methods: </strong>From January 2021 to December 2021, 310 consecutive patients (113 males and 197 females) with 341 pulmonary nodules who underwent CT-guided microcoil or hook-wire localization prior to video-assisted thoracoscopic surgery (VATS) at our center were retrospectively included in this study. There were 161 patients in the microcoil group and 149 patients in the hook-wire group. The successful localization rate, complication rate, radiation exposure, and medical costs were compared between the two groups.</p><p><strong>Results: </strong>A total of 341 pulmonary nodules were localized, with a success rate of 99% (180/184) in the microcoil group and 93% (146/157) in the hook-wire group, respectively. All patients successfully underwent VATS. Multivariate analysis revealed that hook-wire localization, shorter needle depth into the lung tissue and the longer waiting time from localization to VATS were the risk factors for the localization failure. The incidences of pneumothorax in the microcoil group and hook-wire group were 34.8% (56/161) and 34.9% (52/149), respectively (P = 0.983). The incidences of pneumorrhagia were 13% (24/184) and 46.5% (73/157), respectively (P = 0.000). Multivariate analysis revealed that hook-wire localization and greater depth of needle penetration into lung tissue were risk factors for pneumorrhagia.</p><p><strong>Conclusion: </strong>Microcoil localization of pulmonary nodules is superior to hook-wire localization in terms of efficacy and safety. This finding provides insight into priority and broader promotion of microcoil localization.</p>","PeriodicalId":9148,"journal":{"name":"BMC Pulmonary Medicine","volume":"24 1","pages":"492"},"PeriodicalIF":2.8000,"publicationDate":"2024-10-08","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11463161/pdf/","citationCount":"0","resultStr":"{\"title\":\"CT-guided microcoil versus hook-wire localization of pulmonary nodule prior to video-assisted thoracoscopic surgery without fluoroscopic guidance.\",\"authors\":\"Xuedong Sun, Jinxin Fu, Chao Ma, Zhenfei Song, Siwei Yang, Long Jin, Feng Duan\",\"doi\":\"10.1186/s12890-024-03306-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Both microcoils and hook-wires are commonly utilized for preoperative pulmonary nodule localization due to their convenience, but it remains unclear which one should be prioritized for recommendation.</p><p><strong>Aims: </strong>To compare the safety and efficacy of microcoils and hook-wires for pulmonary nodule localization.</p><p><strong>Methods: </strong>From January 2021 to December 2021, 310 consecutive patients (113 males and 197 females) with 341 pulmonary nodules who underwent CT-guided microcoil or hook-wire localization prior to video-assisted thoracoscopic surgery (VATS) at our center were retrospectively included in this study. There were 161 patients in the microcoil group and 149 patients in the hook-wire group. The successful localization rate, complication rate, radiation exposure, and medical costs were compared between the two groups.</p><p><strong>Results: </strong>A total of 341 pulmonary nodules were localized, with a success rate of 99% (180/184) in the microcoil group and 93% (146/157) in the hook-wire group, respectively. All patients successfully underwent VATS. Multivariate analysis revealed that hook-wire localization, shorter needle depth into the lung tissue and the longer waiting time from localization to VATS were the risk factors for the localization failure. The incidences of pneumothorax in the microcoil group and hook-wire group were 34.8% (56/161) and 34.9% (52/149), respectively (P = 0.983). The incidences of pneumorrhagia were 13% (24/184) and 46.5% (73/157), respectively (P = 0.000). Multivariate analysis revealed that hook-wire localization and greater depth of needle penetration into lung tissue were risk factors for pneumorrhagia.</p><p><strong>Conclusion: </strong>Microcoil localization of pulmonary nodules is superior to hook-wire localization in terms of efficacy and safety. This finding provides insight into priority and broader promotion of microcoil localization.</p>\",\"PeriodicalId\":9148,\"journal\":{\"name\":\"BMC Pulmonary Medicine\",\"volume\":\"24 1\",\"pages\":\"492\"},\"PeriodicalIF\":2.8000,\"publicationDate\":\"2024-10-08\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11463161/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"BMC Pulmonary Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12890-024-03306-0\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"RESPIRATORY SYSTEM\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"BMC Pulmonary Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12890-024-03306-0","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"RESPIRATORY SYSTEM","Score":null,"Total":0}
CT-guided microcoil versus hook-wire localization of pulmonary nodule prior to video-assisted thoracoscopic surgery without fluoroscopic guidance.
Background: Both microcoils and hook-wires are commonly utilized for preoperative pulmonary nodule localization due to their convenience, but it remains unclear which one should be prioritized for recommendation.
Aims: To compare the safety and efficacy of microcoils and hook-wires for pulmonary nodule localization.
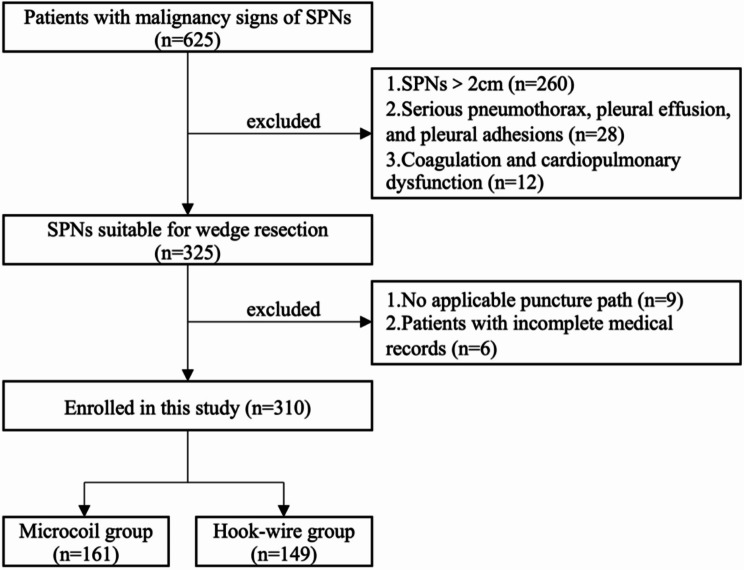
Methods: From January 2021 to December 2021, 310 consecutive patients (113 males and 197 females) with 341 pulmonary nodules who underwent CT-guided microcoil or hook-wire localization prior to video-assisted thoracoscopic surgery (VATS) at our center were retrospectively included in this study. There were 161 patients in the microcoil group and 149 patients in the hook-wire group. The successful localization rate, complication rate, radiation exposure, and medical costs were compared between the two groups.
Results: A total of 341 pulmonary nodules were localized, with a success rate of 99% (180/184) in the microcoil group and 93% (146/157) in the hook-wire group, respectively. All patients successfully underwent VATS. Multivariate analysis revealed that hook-wire localization, shorter needle depth into the lung tissue and the longer waiting time from localization to VATS were the risk factors for the localization failure. The incidences of pneumothorax in the microcoil group and hook-wire group were 34.8% (56/161) and 34.9% (52/149), respectively (P = 0.983). The incidences of pneumorrhagia were 13% (24/184) and 46.5% (73/157), respectively (P = 0.000). Multivariate analysis revealed that hook-wire localization and greater depth of needle penetration into lung tissue were risk factors for pneumorrhagia.
Conclusion: Microcoil localization of pulmonary nodules is superior to hook-wire localization in terms of efficacy and safety. This finding provides insight into priority and broader promotion of microcoil localization.
期刊介绍:
BMC Pulmonary Medicine is an open access, peer-reviewed journal that considers articles on all aspects of the prevention, diagnosis and management of pulmonary and associated disorders, as well as related molecular genetics, pathophysiology, and epidemiology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


