{"title":"开发并验证用于预测接受胸外科手术的老年患者肺部并发症的提名图。","authors":"Jingjing Liu, Dinghao Xue, Long Wang, Yanxiang Li, Luyu Liu, Guosong Liao, Jiangbei Cao, Yanhong Liu, Jingsheng Lou, Hao Li, Yongbin Yang, Weidong Mi, Qiang Fu","doi":"10.1007/s40520-024-02844-1","DOIUrl":null,"url":null,"abstract":"<div><h3>Background</h3><p>Postoperative pulmonary complications (PPCs) remain a prevalent concern among elderly patients undergoing surgery, with a notably higher incidence observed in elderly patients undergoing thoracic surgery. This study aimed to develop a nomogram to predict the risk of PPCs in this population.</p><h3>Methods</h3><p>A total of 2963 elderly patients who underwent thoracic surgery were enrolled and randomly divided into a training cohort (80%, <i>n</i> = 2369) or a validation cohort (20%, <i>n</i> = 593). Univariate and multivariate logistic regression analyses were conducted to identify risk factors for PPCs, and a nomogram was developed based on the findings from the training cohort. The validation cohort was used to validate the model. The predictive accuracy of the model was evaluated by receiver operating characteristic (ROC) curve, area under ROC (AUC), calibration curve, and decision curve analysis (DCA).</p><h3>Results</h3><p>A total of 918 (31.0%) patients reported PPCs. Nine independent risk factors for PPCs were identified: preoperative presence of chronic obstructive pulmonary disease (COPD), elevated leukocyte count, higher partial pressure of arterial carbon dioxide (PaCO<sub>2</sub>) level, surgical site, thoracotomy, intraoperative hypotension, blood loss > 100 mL, surgery duration > 180 min, and malignant tumor. The AUC value for the training cohort was 0.739 (95% <i>CI</i>: 0.719–0.762), and it was 0.703 for the validation cohort (95% <i>CI</i>: 0.657–0.749). The <i>P-</i>values for the Hosmer-Lemeshow test were 0.633 and 0.144 for the training and validation cohorts, respectively, indicating a notable calibration curve fit. The DCA curve indicated that the nomogram could be applied clinically if the risk threshold was between 12% and 84%, which was found to be between 8% and 82% in the validation cohort.</p><h3>Conclusion</h3><p>This study highlighted the pressing need for early detection of PPCs in elderly patients undergoing thoracic surgery. The nomogram exhibited promising predictive efficacy for PPCs in elderly patients undergoing thoracic surgery, enabling the identification of high-risk patients and consequently aiding in the implementation of preventive interventions.</p><h3>Graphical Abstract</h3><div><figure><div><div><picture><img></picture></div></div></figure></div></div>","PeriodicalId":7720,"journal":{"name":"Aging Clinical and Experimental Research","volume":"36 1","pages":""},"PeriodicalIF":3.4000,"publicationDate":"2024-10-05","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11455794/pdf/","citationCount":"0","resultStr":"{\"title\":\"Development and validation of a nomogram for predicting pulmonary complications in elderly patients undergoing thoracic surgery\",\"authors\":\"Jingjing Liu, Dinghao Xue, Long Wang, Yanxiang Li, Luyu Liu, Guosong Liao, Jiangbei Cao, Yanhong Liu, Jingsheng Lou, Hao Li, Yongbin Yang, Weidong Mi, Qiang Fu\",\"doi\":\"10.1007/s40520-024-02844-1\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div><h3>Background</h3><p>Postoperative pulmonary complications (PPCs) remain a prevalent concern among elderly patients undergoing surgery, with a notably higher incidence observed in elderly patients undergoing thoracic surgery. This study aimed to develop a nomogram to predict the risk of PPCs in this population.</p><h3>Methods</h3><p>A total of 2963 elderly patients who underwent thoracic surgery were enrolled and randomly divided into a training cohort (80%, <i>n</i> = 2369) or a validation cohort (20%, <i>n</i> = 593). Univariate and multivariate logistic regression analyses were conducted to identify risk factors for PPCs, and a nomogram was developed based on the findings from the training cohort. The validation cohort was used to validate the model. The predictive accuracy of the model was evaluated by receiver operating characteristic (ROC) curve, area under ROC (AUC), calibration curve, and decision curve analysis (DCA).</p><h3>Results</h3><p>A total of 918 (31.0%) patients reported PPCs. Nine independent risk factors for PPCs were identified: preoperative presence of chronic obstructive pulmonary disease (COPD), elevated leukocyte count, higher partial pressure of arterial carbon dioxide (PaCO<sub>2</sub>) level, surgical site, thoracotomy, intraoperative hypotension, blood loss > 100 mL, surgery duration > 180 min, and malignant tumor. The AUC value for the training cohort was 0.739 (95% <i>CI</i>: 0.719–0.762), and it was 0.703 for the validation cohort (95% <i>CI</i>: 0.657–0.749). The <i>P-</i>values for the Hosmer-Lemeshow test were 0.633 and 0.144 for the training and validation cohorts, respectively, indicating a notable calibration curve fit. The DCA curve indicated that the nomogram could be applied clinically if the risk threshold was between 12% and 84%, which was found to be between 8% and 82% in the validation cohort.</p><h3>Conclusion</h3><p>This study highlighted the pressing need for early detection of PPCs in elderly patients undergoing thoracic surgery. The nomogram exhibited promising predictive efficacy for PPCs in elderly patients undergoing thoracic surgery, enabling the identification of high-risk patients and consequently aiding in the implementation of preventive interventions.</p><h3>Graphical Abstract</h3><div><figure><div><div><picture><img></picture></div></div></figure></div></div>\",\"PeriodicalId\":7720,\"journal\":{\"name\":\"Aging Clinical and Experimental Research\",\"volume\":\"36 1\",\"pages\":\"\"},\"PeriodicalIF\":3.4000,\"publicationDate\":\"2024-10-05\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11455794/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Aging Clinical and Experimental Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://link.springer.com/article/10.1007/s40520-024-02844-1\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GERIATRICS & GERONTOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Aging Clinical and Experimental Research","FirstCategoryId":"3","ListUrlMain":"https://link.springer.com/article/10.1007/s40520-024-02844-1","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GERIATRICS & GERONTOLOGY","Score":null,"Total":0}
Development and validation of a nomogram for predicting pulmonary complications in elderly patients undergoing thoracic surgery
Background
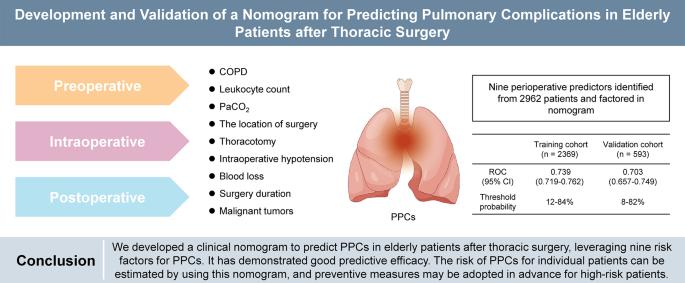
Postoperative pulmonary complications (PPCs) remain a prevalent concern among elderly patients undergoing surgery, with a notably higher incidence observed in elderly patients undergoing thoracic surgery. This study aimed to develop a nomogram to predict the risk of PPCs in this population.
Methods
A total of 2963 elderly patients who underwent thoracic surgery were enrolled and randomly divided into a training cohort (80%, n = 2369) or a validation cohort (20%, n = 593). Univariate and multivariate logistic regression analyses were conducted to identify risk factors for PPCs, and a nomogram was developed based on the findings from the training cohort. The validation cohort was used to validate the model. The predictive accuracy of the model was evaluated by receiver operating characteristic (ROC) curve, area under ROC (AUC), calibration curve, and decision curve analysis (DCA).
Results
A total of 918 (31.0%) patients reported PPCs. Nine independent risk factors for PPCs were identified: preoperative presence of chronic obstructive pulmonary disease (COPD), elevated leukocyte count, higher partial pressure of arterial carbon dioxide (PaCO2) level, surgical site, thoracotomy, intraoperative hypotension, blood loss > 100 mL, surgery duration > 180 min, and malignant tumor. The AUC value for the training cohort was 0.739 (95% CI: 0.719–0.762), and it was 0.703 for the validation cohort (95% CI: 0.657–0.749). The P-values for the Hosmer-Lemeshow test were 0.633 and 0.144 for the training and validation cohorts, respectively, indicating a notable calibration curve fit. The DCA curve indicated that the nomogram could be applied clinically if the risk threshold was between 12% and 84%, which was found to be between 8% and 82% in the validation cohort.
Conclusion
This study highlighted the pressing need for early detection of PPCs in elderly patients undergoing thoracic surgery. The nomogram exhibited promising predictive efficacy for PPCs in elderly patients undergoing thoracic surgery, enabling the identification of high-risk patients and consequently aiding in the implementation of preventive interventions.
期刊介绍:
Aging clinical and experimental research offers a multidisciplinary forum on the progressing field of gerontology and geriatrics. The areas covered by the journal include: biogerontology, neurosciences, epidemiology, clinical gerontology and geriatric assessment, social, economical and behavioral gerontology. “Aging clinical and experimental research” appears bimonthly and publishes review articles, original papers and case reports.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


