Maria Lembo, Maria Virginia Manzi, Daniela Pacella, Raffaele Piccolo, Maria Angela Losi, Grazia Canciello, Costantino Mancusi, Luca Bardi, Giuseppe Giugliano, Carmine Morisco, Bruno Trimarco, Daniela Carnevale, Raffaele Izzo, Eduardo Bossone, Giovanni Esposito
{"title":"延长降压治疗时间会加重动脉高血压的器官损伤和血压控制。","authors":"Maria Lembo, Maria Virginia Manzi, Daniela Pacella, Raffaele Piccolo, Maria Angela Losi, Grazia Canciello, Costantino Mancusi, Luca Bardi, Giuseppe Giugliano, Carmine Morisco, Bruno Trimarco, Daniela Carnevale, Raffaele Izzo, Eduardo Bossone, Giovanni Esposito","doi":"10.1007/s40292-024-00673-x","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Delay in arterial hypertension (AH) diagnosis and late therapy initiation may affect progression towards hypertensive-mediated organ damage (HMOD) and blood pressure (BP) control.</p><p><strong>Aim: </strong>We aimed to assess the impact of time-to-therapy on BP control and HMOD in patients receiving AH diagnosis.</p><p><strong>Methods: </strong>We analysed data from the Campania Salute Network, a prospective registry of hypertensive patients (NCT02211365). At baseline visit, time-to-therapy was defined as the interval between the first occurrence of BP values exceeding guidelines-directed thresholds and therapy initiation; HMOD included left ventricular hypertrophy (LVH), carotid plaque, or chronic kidney disease. Optimal BP control was considered for average values < 140/90 mmHg. Low-risk profile was defined as grade I AH without additional cardiovascular risk factors.</p><p><strong>Results: </strong>From 14,161 hypertensive patients, we selected 1,627 participants who were not on antihypertensive therapy. This population was divided into two groups based on the median time-to-therapy (≤ 2 years n = 1,009, > 2 years n = 618). Patients with a time-to-therapy > 2 years had higher risk of HMOD (adjusted odds ratio, aOR:1.51, 95%, CI:1.19-1.93, p < 0.001) due to increased risks of LVH (aOR:1.43, CI:1.12-1.82, p = 0.004), carotid plaques (aOR:1.29, CI:1.00-1.65, p = 0.047), and chronic kidney disease (aOR:1.68, CI:1.08-2.62, p = 0.022). Time-to-therapy > 2 years was significantly associated with uncontrolled BP values (aOR:1.49, CI:1.18-1.88, p < 0.001) and higher number of antihypertensive drugs (aOR:1.68, CI:1.36-2.08, p < 0.001) during follow-up. In low-risk subgroup, time-to-therapy > 2 years did not impact on BP control and number of drugs.</p><p><strong>Conclusions: </strong>In hypertensive patients, a time-to-therapy > 2 years is associated with HMOD and uncontrolled BP.</p>","PeriodicalId":12890,"journal":{"name":"High Blood Pressure & Cardiovascular Prevention","volume":" ","pages":"639-648"},"PeriodicalIF":2.9000,"publicationDate":"2024-11-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11604795/pdf/","citationCount":"0","resultStr":"{\"title\":\"Prolonged Time-to-antihypertensive Therapy Worsens Organ Damage and Blood Pressure Control in Arterial Hypertension.\",\"authors\":\"Maria Lembo, Maria Virginia Manzi, Daniela Pacella, Raffaele Piccolo, Maria Angela Losi, Grazia Canciello, Costantino Mancusi, Luca Bardi, Giuseppe Giugliano, Carmine Morisco, Bruno Trimarco, Daniela Carnevale, Raffaele Izzo, Eduardo Bossone, Giovanni Esposito\",\"doi\":\"10.1007/s40292-024-00673-x\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Delay in arterial hypertension (AH) diagnosis and late therapy initiation may affect progression towards hypertensive-mediated organ damage (HMOD) and blood pressure (BP) control.</p><p><strong>Aim: </strong>We aimed to assess the impact of time-to-therapy on BP control and HMOD in patients receiving AH diagnosis.</p><p><strong>Methods: </strong>We analysed data from the Campania Salute Network, a prospective registry of hypertensive patients (NCT02211365). At baseline visit, time-to-therapy was defined as the interval between the first occurrence of BP values exceeding guidelines-directed thresholds and therapy initiation; HMOD included left ventricular hypertrophy (LVH), carotid plaque, or chronic kidney disease. Optimal BP control was considered for average values < 140/90 mmHg. Low-risk profile was defined as grade I AH without additional cardiovascular risk factors.</p><p><strong>Results: </strong>From 14,161 hypertensive patients, we selected 1,627 participants who were not on antihypertensive therapy. This population was divided into two groups based on the median time-to-therapy (≤ 2 years n = 1,009, > 2 years n = 618). Patients with a time-to-therapy > 2 years had higher risk of HMOD (adjusted odds ratio, aOR:1.51, 95%, CI:1.19-1.93, p < 0.001) due to increased risks of LVH (aOR:1.43, CI:1.12-1.82, p = 0.004), carotid plaques (aOR:1.29, CI:1.00-1.65, p = 0.047), and chronic kidney disease (aOR:1.68, CI:1.08-2.62, p = 0.022). Time-to-therapy > 2 years was significantly associated with uncontrolled BP values (aOR:1.49, CI:1.18-1.88, p < 0.001) and higher number of antihypertensive drugs (aOR:1.68, CI:1.36-2.08, p < 0.001) during follow-up. In low-risk subgroup, time-to-therapy > 2 years did not impact on BP control and number of drugs.</p><p><strong>Conclusions: </strong>In hypertensive patients, a time-to-therapy > 2 years is associated with HMOD and uncontrolled BP.</p>\",\"PeriodicalId\":12890,\"journal\":{\"name\":\"High Blood Pressure & Cardiovascular Prevention\",\"volume\":\" \",\"pages\":\"639-648\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-11-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11604795/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"High Blood Pressure & Cardiovascular Prevention\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1007/s40292-024-00673-x\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/10/5 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q2\",\"JCRName\":\"PERIPHERAL VASCULAR DISEASE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"High Blood Pressure & Cardiovascular Prevention","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1007/s40292-024-00673-x","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/10/5 0:00:00","PubModel":"Epub","JCR":"Q2","JCRName":"PERIPHERAL VASCULAR DISEASE","Score":null,"Total":0}
Prolonged Time-to-antihypertensive Therapy Worsens Organ Damage and Blood Pressure Control in Arterial Hypertension.
Introduction: Delay in arterial hypertension (AH) diagnosis and late therapy initiation may affect progression towards hypertensive-mediated organ damage (HMOD) and blood pressure (BP) control.
Aim: We aimed to assess the impact of time-to-therapy on BP control and HMOD in patients receiving AH diagnosis.
Methods: We analysed data from the Campania Salute Network, a prospective registry of hypertensive patients (NCT02211365). At baseline visit, time-to-therapy was defined as the interval between the first occurrence of BP values exceeding guidelines-directed thresholds and therapy initiation; HMOD included left ventricular hypertrophy (LVH), carotid plaque, or chronic kidney disease. Optimal BP control was considered for average values < 140/90 mmHg. Low-risk profile was defined as grade I AH without additional cardiovascular risk factors.
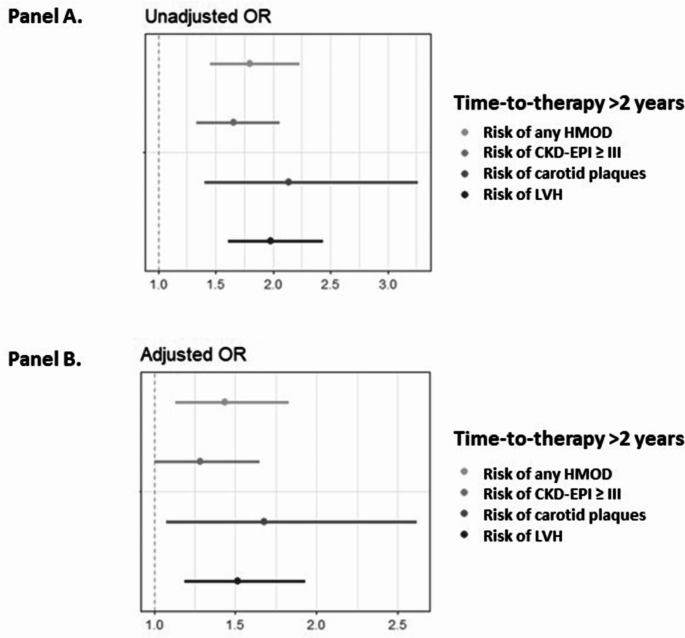
Results: From 14,161 hypertensive patients, we selected 1,627 participants who were not on antihypertensive therapy. This population was divided into two groups based on the median time-to-therapy (≤ 2 years n = 1,009, > 2 years n = 618). Patients with a time-to-therapy > 2 years had higher risk of HMOD (adjusted odds ratio, aOR:1.51, 95%, CI:1.19-1.93, p < 0.001) due to increased risks of LVH (aOR:1.43, CI:1.12-1.82, p = 0.004), carotid plaques (aOR:1.29, CI:1.00-1.65, p = 0.047), and chronic kidney disease (aOR:1.68, CI:1.08-2.62, p = 0.022). Time-to-therapy > 2 years was significantly associated with uncontrolled BP values (aOR:1.49, CI:1.18-1.88, p < 0.001) and higher number of antihypertensive drugs (aOR:1.68, CI:1.36-2.08, p < 0.001) during follow-up. In low-risk subgroup, time-to-therapy > 2 years did not impact on BP control and number of drugs.
Conclusions: In hypertensive patients, a time-to-therapy > 2 years is associated with HMOD and uncontrolled BP.
期刊介绍:
High Blood Pressure & Cardiovascular Prevention promotes knowledge, update and discussion in the field of hypertension and cardiovascular disease prevention, by providing a regular programme of independent review articles covering key aspects of the management of hypertension and cardiovascular diseases. The journal includes: Invited ''State of the Art'' reviews. Expert commentaries on guidelines, major trials, technical advances.Presentation of new intervention trials design.''Pros and Cons'' or round tables on controversial issues.Statements on guidelines from hypertension and cardiovascular scientific societies.Socio-economic issues.Cost/benefit in prevention of cardiovascular diseases.Monitoring of healthcare systems.News and views from the Italian Society of Hypertension (including abstracts).All manuscripts are subject to peer review by international experts. Letters to the editor are welcomed and will be considered for publication.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


