Nannan Jiang, Li Xiang, Huijie Huang, Xudong Zhang
{"title":"用生物制剂治疗中国儿童运动诱发的过敏性休克:病例报告。","authors":"Nannan Jiang, Li Xiang, Huijie Huang, Xudong Zhang","doi":"10.3389/falgy.2024.1453873","DOIUrl":null,"url":null,"abstract":"<p><p>Exercise-induced anaphylaxis (EIA) is a rare and potentially life-threatening disorder. In difficult to control and refractory cases of EIA, biologics such as omalizumab and dupilumab have shown promise, with documented successful outcomes. Here, we present a case of EIA with lipid transfer protein (LTP) sensitization successfully treated with omalizumab with long-term follow-up. A 12-year-old girl presented to our allergy department because of recurrent episodes of EIA, with no specific food ingestion before exercise. Allergen testing revealed sensitization to weed pollens, particularly mugwort (76.1 kUA/L) and <i>Alternaria alternata</i> (10.8 kUA/L). Allergen component testing indicated sensitization to LTP components from mugwort Art v 3 (49.9 kUA/L), wheat Tri a 14 (2.03 kUA/L), and peach Pru p 3 (11.5 kUA/L), with a negative result for omega-5 gliadin. Despite initial prophylactic treatment with budesonide-formoterol (80/4.5 μg) and cetirizine (10 mg) before exercise, the patient still experienced EIA; she was then recommended for dupilumab therapy (an initial dose of 600 mg, followed by 300 mg every 2 weeks for six doses). However, even while undergoing dupilumab therapy, she suffered two anaphylactic episodes after running 800-1,000 m. With the patient's consent, a trial of omalizumab was initiated (injections of 300 mg every 4 weeks). After 2 months of omalizumab therapy, the patient showed significant improvement. She had been engaging in physical exercise three times a week and experienced a mild episode of urticaria. There were no further episodes of anaphylaxis or emergency room visits. By the fourth month of omalizumab treatment, she was able to consume food normally even just before exercising and had returned to her full activity level without any restrictions. This case presents the first successful off-label use of omalizumab in the prevention of EIA in the Chinese population. It is concluded that omalizumab may be helpful in resolving EIA symptoms, as evidenced by this case of successful long-term use.</p>","PeriodicalId":73062,"journal":{"name":"Frontiers in allergy","volume":"5 ","pages":"1453873"},"PeriodicalIF":3.1000,"publicationDate":"2024-09-19","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11446895/pdf/","citationCount":"0","resultStr":"{\"title\":\"The management of exercise-induced anaphylaxis in a Chinese child with biologics: a case report.\",\"authors\":\"Nannan Jiang, Li Xiang, Huijie Huang, Xudong Zhang\",\"doi\":\"10.3389/falgy.2024.1453873\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Exercise-induced anaphylaxis (EIA) is a rare and potentially life-threatening disorder. In difficult to control and refractory cases of EIA, biologics such as omalizumab and dupilumab have shown promise, with documented successful outcomes. Here, we present a case of EIA with lipid transfer protein (LTP) sensitization successfully treated with omalizumab with long-term follow-up. A 12-year-old girl presented to our allergy department because of recurrent episodes of EIA, with no specific food ingestion before exercise. Allergen testing revealed sensitization to weed pollens, particularly mugwort (76.1 kUA/L) and <i>Alternaria alternata</i> (10.8 kUA/L). Allergen component testing indicated sensitization to LTP components from mugwort Art v 3 (49.9 kUA/L), wheat Tri a 14 (2.03 kUA/L), and peach Pru p 3 (11.5 kUA/L), with a negative result for omega-5 gliadin. Despite initial prophylactic treatment with budesonide-formoterol (80/4.5 μg) and cetirizine (10 mg) before exercise, the patient still experienced EIA; she was then recommended for dupilumab therapy (an initial dose of 600 mg, followed by 300 mg every 2 weeks for six doses). However, even while undergoing dupilumab therapy, she suffered two anaphylactic episodes after running 800-1,000 m. With the patient's consent, a trial of omalizumab was initiated (injections of 300 mg every 4 weeks). After 2 months of omalizumab therapy, the patient showed significant improvement. She had been engaging in physical exercise three times a week and experienced a mild episode of urticaria. There were no further episodes of anaphylaxis or emergency room visits. By the fourth month of omalizumab treatment, she was able to consume food normally even just before exercising and had returned to her full activity level without any restrictions. This case presents the first successful off-label use of omalizumab in the prevention of EIA in the Chinese population. It is concluded that omalizumab may be helpful in resolving EIA symptoms, as evidenced by this case of successful long-term use.</p>\",\"PeriodicalId\":73062,\"journal\":{\"name\":\"Frontiers in allergy\",\"volume\":\"5 \",\"pages\":\"1453873\"},\"PeriodicalIF\":3.1000,\"publicationDate\":\"2024-09-19\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11446895/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Frontiers in allergy\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3389/falgy.2024.1453873\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q2\",\"JCRName\":\"ALLERGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Frontiers in allergy","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3389/falgy.2024.1453873","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q2","JCRName":"ALLERGY","Score":null,"Total":0}
引用次数: 0
摘要
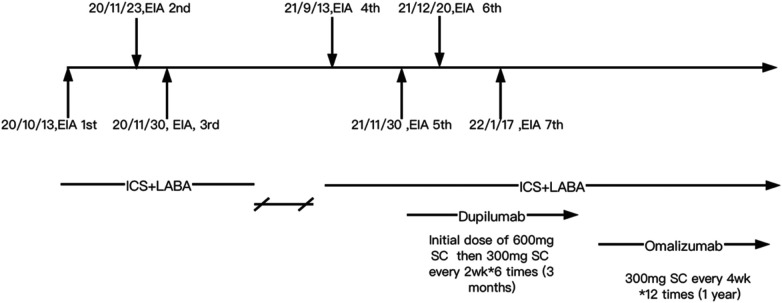
运动诱发过敏性休克(EIA)是一种罕见且可能危及生命的疾病。对于难以控制和难治的 EIA 病例,奥马珠单抗和杜比鲁单抗等生物制剂已显示出治疗前景,并取得了有据可查的成功结果。在此,我们介绍一例使用奥马珠单抗成功治疗并长期随访的伴有脂质转移蛋白(LTP)致敏的 EIA 病例。一名 12 岁女孩因反复发作 EIA 而到过敏科就诊,运动前未摄入特定食物。过敏原检测显示她对杂草花粉过敏,尤其是艾草(76.1 kUA/L)和交替孢霉(10.8 kUA/L)。过敏原成分检测显示,患者对艾蒿 Art v 3(49.9 kUA/L)、小麦 Tri a 14(2.03 kUA/L)和桃子 Pru p 3(11.5 kUA/L)中的 LTP 成分过敏,而对Ω-5 胶质蛋白的检测结果为阴性。尽管在运动前使用布地奈德-福莫特罗(80/4.5 μg)和西替利嗪(10 mg)进行了初步预防性治疗,但患者仍出现了 EIA;随后,医生建议她接受杜比卢单抗治疗(初始剂量为 600 mg,之后每 2 周服用 300 mg,共服用 6 次)。然而,即使在接受双鲁单抗治疗期间,她在跑步 800-1000 米后仍两次出现过敏反应。在征得患者同意后,开始试用奥马珠单抗(每 4 周注射一次,每次 300 毫克)。经过两个月的奥马珠单抗治疗,患者的病情有了明显好转。她每周进行三次体育锻炼,并经历了一次轻微的荨麻疹发作。此后没有再出现过敏性休克或急诊就诊。在奥马珠单抗治疗的第四个月,她甚至在运动前也能正常进食,并恢复到完全活动水平,没有受到任何限制。本病例是奥马珠单抗首次在标签外成功用于中国人群的 EIA 预防。结论是,奥马珠单抗可能有助于缓解 EIA 症状,本病例的长期成功使用就是证明。
The management of exercise-induced anaphylaxis in a Chinese child with biologics: a case report.
Exercise-induced anaphylaxis (EIA) is a rare and potentially life-threatening disorder. In difficult to control and refractory cases of EIA, biologics such as omalizumab and dupilumab have shown promise, with documented successful outcomes. Here, we present a case of EIA with lipid transfer protein (LTP) sensitization successfully treated with omalizumab with long-term follow-up. A 12-year-old girl presented to our allergy department because of recurrent episodes of EIA, with no specific food ingestion before exercise. Allergen testing revealed sensitization to weed pollens, particularly mugwort (76.1 kUA/L) and Alternaria alternata (10.8 kUA/L). Allergen component testing indicated sensitization to LTP components from mugwort Art v 3 (49.9 kUA/L), wheat Tri a 14 (2.03 kUA/L), and peach Pru p 3 (11.5 kUA/L), with a negative result for omega-5 gliadin. Despite initial prophylactic treatment with budesonide-formoterol (80/4.5 μg) and cetirizine (10 mg) before exercise, the patient still experienced EIA; she was then recommended for dupilumab therapy (an initial dose of 600 mg, followed by 300 mg every 2 weeks for six doses). However, even while undergoing dupilumab therapy, she suffered two anaphylactic episodes after running 800-1,000 m. With the patient's consent, a trial of omalizumab was initiated (injections of 300 mg every 4 weeks). After 2 months of omalizumab therapy, the patient showed significant improvement. She had been engaging in physical exercise three times a week and experienced a mild episode of urticaria. There were no further episodes of anaphylaxis or emergency room visits. By the fourth month of omalizumab treatment, she was able to consume food normally even just before exercising and had returned to her full activity level without any restrictions. This case presents the first successful off-label use of omalizumab in the prevention of EIA in the Chinese population. It is concluded that omalizumab may be helpful in resolving EIA symptoms, as evidenced by this case of successful long-term use.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


