Nina Nouhravesh, Stephen J. Greene, Robert Clare, Daniel Wojdyla, Kevin J. Anstrom, Eric Velazquez, Bertram Pitt, Robert J. Mentz, Mitchell A. Psotka
{"title":"心力衰竭住院后使用托塞米和呋塞米的利尿剂剂量和疗效:TRANSFORM-HF 试验。","authors":"Nina Nouhravesh, Stephen J. Greene, Robert Clare, Daniel Wojdyla, Kevin J. Anstrom, Eric Velazquez, Bertram Pitt, Robert J. Mentz, Mitchell A. Psotka","doi":"10.1002/ejhf.3458","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aims</h3>\n \n <p>The TRANSFORM-HF trial found no difference in clinical outcomes between torsemide versus furosemide after hospitalization for heart failure. This analysis aimed to assess the impact of diuretic dosing on the primary and secondary clinical outcomes.</p>\n </section>\n \n <section>\n \n <h3> Methods and results</h3>\n \n <p>This post-hoc analysis of TRANSFORM-HF categorized patients into three groups by discharge diuretic dose: (1) ≤40 mg, (2) >40–80 mg, and (3) >80 mg of furosemide equivalents. The associations between discharge dose and 12-month clinical events, and change in Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CSS), were assessed. Overall, 2379 patients were included, aged 65 years (interquartile range 56–75), 883 (37.1%) women, and 812 (34.2%) Black. Furosemide had adjusted hazard ratios (aHR) for all-cause mortality of 1.21 (95% confidence interval [CI] 0.91–1.59) for discharge dose group 2 and 1.40 (95% CI 1.04–1.88) for group 3, compared with group 1. For torsemide, aHRs were 1.74 (95% CI 1.32–2.30) for group 2 and 1.58 (95% CI 1.14–2.19) for group 3. No evidence of heterogeneity for the association between increased mortality and higher dose was found by loop diuretic type (<i>p</i><sub>interaction</sub> = 0.17). Higher doses of furosemide and torsemide were associated with increased risk of all-cause hospitalization and the composite of all-cause mortality and hospitalization, without evidence of heterogeneity by loop diuretic type (<i>p</i><sub>interaction</sub> > 0.2). Changes in KCCQ-CSS from baseline at 12 months was similar across dose groups for both drugs.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>Following hospitalization for heart failure, higher loop diuretic dosing was independently associated with worse clinical and patient-reported outcomes. The correlation between higher loop diuretic dose and outcomes was consistent, regardless of loop diuretic used.</p>\n </section>\n </div>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":"27 2","pages":"317-324"},"PeriodicalIF":16.9000,"publicationDate":"2024-10-04","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Diuretic dosing and outcomes with torsemide and furosemide following hospitalization for heart failure: The TRANSFORM-HF trial\",\"authors\":\"Nina Nouhravesh, Stephen J. Greene, Robert Clare, Daniel Wojdyla, Kevin J. Anstrom, Eric Velazquez, Bertram Pitt, Robert J. Mentz, Mitchell A. Psotka\",\"doi\":\"10.1002/ejhf.3458\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aims</h3>\\n \\n <p>The TRANSFORM-HF trial found no difference in clinical outcomes between torsemide versus furosemide after hospitalization for heart failure. This analysis aimed to assess the impact of diuretic dosing on the primary and secondary clinical outcomes.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods and results</h3>\\n \\n <p>This post-hoc analysis of TRANSFORM-HF categorized patients into three groups by discharge diuretic dose: (1) ≤40 mg, (2) >40–80 mg, and (3) >80 mg of furosemide equivalents. The associations between discharge dose and 12-month clinical events, and change in Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CSS), were assessed. Overall, 2379 patients were included, aged 65 years (interquartile range 56–75), 883 (37.1%) women, and 812 (34.2%) Black. Furosemide had adjusted hazard ratios (aHR) for all-cause mortality of 1.21 (95% confidence interval [CI] 0.91–1.59) for discharge dose group 2 and 1.40 (95% CI 1.04–1.88) for group 3, compared with group 1. For torsemide, aHRs were 1.74 (95% CI 1.32–2.30) for group 2 and 1.58 (95% CI 1.14–2.19) for group 3. No evidence of heterogeneity for the association between increased mortality and higher dose was found by loop diuretic type (<i>p</i><sub>interaction</sub> = 0.17). Higher doses of furosemide and torsemide were associated with increased risk of all-cause hospitalization and the composite of all-cause mortality and hospitalization, without evidence of heterogeneity by loop diuretic type (<i>p</i><sub>interaction</sub> > 0.2). Changes in KCCQ-CSS from baseline at 12 months was similar across dose groups for both drugs.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>Following hospitalization for heart failure, higher loop diuretic dosing was independently associated with worse clinical and patient-reported outcomes. The correlation between higher loop diuretic dose and outcomes was consistent, regardless of loop diuretic used.</p>\\n </section>\\n </div>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\"27 2\",\"pages\":\"317-324\"},\"PeriodicalIF\":16.9000,\"publicationDate\":\"2024-10-04\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3458\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1002/ejhf.3458","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
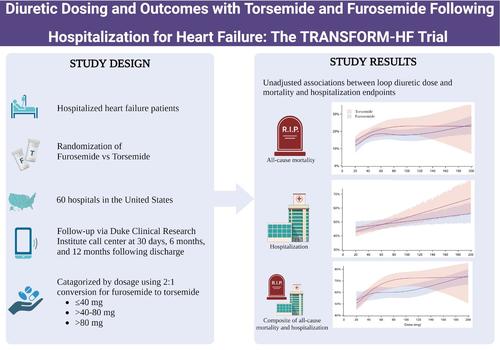
Diuretic dosing and outcomes with torsemide and furosemide following hospitalization for heart failure: The TRANSFORM-HF trial
Aims
The TRANSFORM-HF trial found no difference in clinical outcomes between torsemide versus furosemide after hospitalization for heart failure. This analysis aimed to assess the impact of diuretic dosing on the primary and secondary clinical outcomes.
Methods and results
This post-hoc analysis of TRANSFORM-HF categorized patients into three groups by discharge diuretic dose: (1) ≤40 mg, (2) >40–80 mg, and (3) >80 mg of furosemide equivalents. The associations between discharge dose and 12-month clinical events, and change in Kansas City Cardiomyopathy Questionnaire clinical summary score (KCCQ-CSS), were assessed. Overall, 2379 patients were included, aged 65 years (interquartile range 56–75), 883 (37.1%) women, and 812 (34.2%) Black. Furosemide had adjusted hazard ratios (aHR) for all-cause mortality of 1.21 (95% confidence interval [CI] 0.91–1.59) for discharge dose group 2 and 1.40 (95% CI 1.04–1.88) for group 3, compared with group 1. For torsemide, aHRs were 1.74 (95% CI 1.32–2.30) for group 2 and 1.58 (95% CI 1.14–2.19) for group 3. No evidence of heterogeneity for the association between increased mortality and higher dose was found by loop diuretic type (pinteraction = 0.17). Higher doses of furosemide and torsemide were associated with increased risk of all-cause hospitalization and the composite of all-cause mortality and hospitalization, without evidence of heterogeneity by loop diuretic type (pinteraction > 0.2). Changes in KCCQ-CSS from baseline at 12 months was similar across dose groups for both drugs.
Conclusion
Following hospitalization for heart failure, higher loop diuretic dosing was independently associated with worse clinical and patient-reported outcomes. The correlation between higher loop diuretic dose and outcomes was consistent, regardless of loop diuretic used.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


