Davut Dayan, Marinus Schmid, Florian K Ebner, Wolfgang Janni, Frank Reister, Beate Hüner, Krisztian Lato, Ulrike Friebe-Hoffmann, Stefan Lukac
{"title":"腹腔镜经腹无针紧急宫腔粘连术在经阴道宫腔粘连术失败后的妊娠早期第二孕期应用:两例病例报告及文献综述。","authors":"Davut Dayan, Marinus Schmid, Florian K Ebner, Wolfgang Janni, Frank Reister, Beate Hüner, Krisztian Lato, Ulrike Friebe-Hoffmann, Stefan Lukac","doi":"10.1055/a-2373-0639","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>The aim of the study was to describe the preventive option and safety of laparoscopic transabdominal emergency cerclage in pregnant women with advanced cervical shortening after failed vaginal cerclage or in whom vaginal cerclage is no longer possible.</p><p><strong>Method: </strong>Laparoscopic isthmo-cervical emergency cerclage was carried out in two patients at 13+0 and 15+5 weeks of gestation (GW) respectively. Both patients had cervical shortening and it was no longer possible to expose the cervix after conization or re-conization. The attempts to carry out transvaginal cerclage were unsuccessful. The technical aspects, feasibility, safety, and pregnancy outcomes after laparoscopic transabdominal cerclage are presented here, based on two case reports.</p><p><strong>Results: </strong>The cerclages were placed after blunt dissection of the uterine vessels and careful introduction of a KELLY forceps through the avascular space between the ascending and descending branches of the uterine vessels without using a needle. The operating times were 93 and 134 minutes (min), respectively. The estimated blood loss during the procedure was less than 50 ml and neither perioperative nor postoperative complications occurred. The subsequent course of both pregnancies was uneventful and fetal development in both cases was normal. In the first case, the baby was delivered by secondary cesarean section following premature rupture of membranes in week 35+4 of gestation. The baby had a birthweight of 2786 g, APGAR scores of 8/9/10 and an umbilical cord arterial pH of 7.36. In the second case, delivery was by primary cesarean section in week 39+5 of gestation. The infant had a birth weight of 4160 g, APGAR scores of 5/9/10 and an umbilical cord arterial pH of 7.20.</p><p><strong>Conclusion: </strong>Laparoscopic transabdominal cerclage is a safe and effective treatment option, even early in the second trimester of pregnancy, for patients in whom transvaginal cerclage is no longer possible due to anatomical factors. The method is technically very feasible and is associated with positive obstetric outcomes. The overall risk of perioperative complications is within acceptable limits.</p>","PeriodicalId":12481,"journal":{"name":"Geburtshilfe Und Frauenheilkunde","volume":"84 10","pages":"989-998"},"PeriodicalIF":1.9000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444752/pdf/","citationCount":"0","resultStr":"{\"title\":\"Laparoscopic Transabdominal Needle-free Emergency Cerclage in the Early Second Trimester of Pregnancy after Failed Transvaginal Cerclage: Two Case Reports and a Review of the Literature.\",\"authors\":\"Davut Dayan, Marinus Schmid, Florian K Ebner, Wolfgang Janni, Frank Reister, Beate Hüner, Krisztian Lato, Ulrike Friebe-Hoffmann, Stefan Lukac\",\"doi\":\"10.1055/a-2373-0639\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>The aim of the study was to describe the preventive option and safety of laparoscopic transabdominal emergency cerclage in pregnant women with advanced cervical shortening after failed vaginal cerclage or in whom vaginal cerclage is no longer possible.</p><p><strong>Method: </strong>Laparoscopic isthmo-cervical emergency cerclage was carried out in two patients at 13+0 and 15+5 weeks of gestation (GW) respectively. Both patients had cervical shortening and it was no longer possible to expose the cervix after conization or re-conization. The attempts to carry out transvaginal cerclage were unsuccessful. The technical aspects, feasibility, safety, and pregnancy outcomes after laparoscopic transabdominal cerclage are presented here, based on two case reports.</p><p><strong>Results: </strong>The cerclages were placed after blunt dissection of the uterine vessels and careful introduction of a KELLY forceps through the avascular space between the ascending and descending branches of the uterine vessels without using a needle. The operating times were 93 and 134 minutes (min), respectively. The estimated blood loss during the procedure was less than 50 ml and neither perioperative nor postoperative complications occurred. The subsequent course of both pregnancies was uneventful and fetal development in both cases was normal. In the first case, the baby was delivered by secondary cesarean section following premature rupture of membranes in week 35+4 of gestation. The baby had a birthweight of 2786 g, APGAR scores of 8/9/10 and an umbilical cord arterial pH of 7.36. In the second case, delivery was by primary cesarean section in week 39+5 of gestation. The infant had a birth weight of 4160 g, APGAR scores of 5/9/10 and an umbilical cord arterial pH of 7.20.</p><p><strong>Conclusion: </strong>Laparoscopic transabdominal cerclage is a safe and effective treatment option, even early in the second trimester of pregnancy, for patients in whom transvaginal cerclage is no longer possible due to anatomical factors. The method is technically very feasible and is associated with positive obstetric outcomes. The overall risk of perioperative complications is within acceptable limits.</p>\",\"PeriodicalId\":12481,\"journal\":{\"name\":\"Geburtshilfe Und Frauenheilkunde\",\"volume\":\"84 10\",\"pages\":\"989-998\"},\"PeriodicalIF\":1.9000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444752/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Geburtshilfe Und Frauenheilkunde\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1055/a-2373-0639\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"OBSTETRICS & GYNECOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Geburtshilfe Und Frauenheilkunde","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1055/a-2373-0639","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"OBSTETRICS & GYNECOLOGY","Score":null,"Total":0}
Laparoscopic Transabdominal Needle-free Emergency Cerclage in the Early Second Trimester of Pregnancy after Failed Transvaginal Cerclage: Two Case Reports and a Review of the Literature.
Purpose: The aim of the study was to describe the preventive option and safety of laparoscopic transabdominal emergency cerclage in pregnant women with advanced cervical shortening after failed vaginal cerclage or in whom vaginal cerclage is no longer possible.
Method: Laparoscopic isthmo-cervical emergency cerclage was carried out in two patients at 13+0 and 15+5 weeks of gestation (GW) respectively. Both patients had cervical shortening and it was no longer possible to expose the cervix after conization or re-conization. The attempts to carry out transvaginal cerclage were unsuccessful. The technical aspects, feasibility, safety, and pregnancy outcomes after laparoscopic transabdominal cerclage are presented here, based on two case reports.
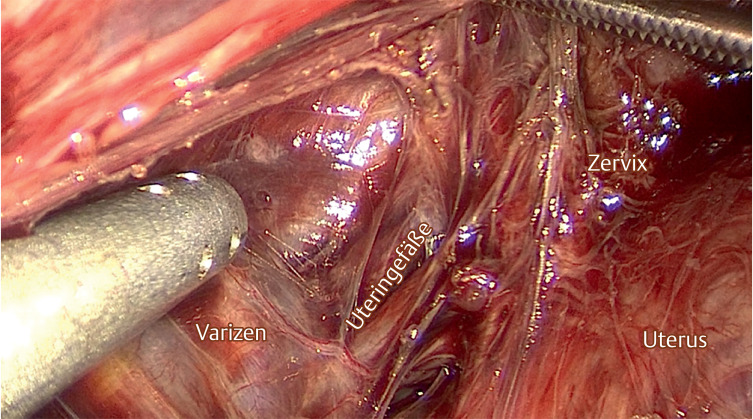
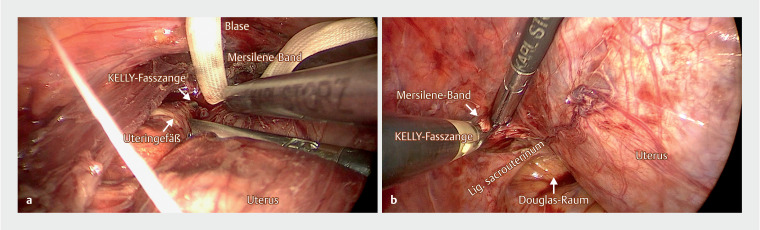
Results: The cerclages were placed after blunt dissection of the uterine vessels and careful introduction of a KELLY forceps through the avascular space between the ascending and descending branches of the uterine vessels without using a needle. The operating times were 93 and 134 minutes (min), respectively. The estimated blood loss during the procedure was less than 50 ml and neither perioperative nor postoperative complications occurred. The subsequent course of both pregnancies was uneventful and fetal development in both cases was normal. In the first case, the baby was delivered by secondary cesarean section following premature rupture of membranes in week 35+4 of gestation. The baby had a birthweight of 2786 g, APGAR scores of 8/9/10 and an umbilical cord arterial pH of 7.36. In the second case, delivery was by primary cesarean section in week 39+5 of gestation. The infant had a birth weight of 4160 g, APGAR scores of 5/9/10 and an umbilical cord arterial pH of 7.20.
Conclusion: Laparoscopic transabdominal cerclage is a safe and effective treatment option, even early in the second trimester of pregnancy, for patients in whom transvaginal cerclage is no longer possible due to anatomical factors. The method is technically very feasible and is associated with positive obstetric outcomes. The overall risk of perioperative complications is within acceptable limits.
期刊介绍:
Geburtshilfe und Frauenheilkunde (GebFra) addresses the whole field of obstetrics and gynecology and is concerned with research as much as with clinical practice. In its scientific section, it publishes original articles, reviews and case reports in all fields of the discipline, namely
gynecological oncology, including oncology of the breast
obstetrics and perinatal medicine,
reproductive medicine,
and urogynecology.
GebFra invites the submission of original articles and review articles.
In addition, the journal publishes guidelines, statements and recommendations in cooperation with the DGGG, SGGG, OEGGG and the Arbeitsgemeinschaft der Wissenschaftlichen Medizinischen Fachgesellschaften (AWMF, Association of Scientific Medical Societies, www.awmf.org). Apart from the scientific section, Geburtshilfe und Frauenheilkunde has a news and views section that also includes discussions, book reviews and professional information.
Letters to the editors are welcome. If a letter discusses an article that has been published in our journal, the corresponding author of the article will be informed and invited to comment on the letter. The comment will be published along with the letter.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


