{"title":"一名成人并发腹膜和胸膜结核:病例报告和文献综述。","authors":"Elham Barahimi, Zahra Ghaeini Hesarooeyeh, Ayoub Basham, Mohadeseh Karimi, Behnoush Heidari","doi":"10.22088/cjim.15.4.735","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The simultaneous involvement of the pleura and peritoneum with tuberculosis in the absence of pulmonary foci is an uncommon condition that may lead physicians to misdiagnose.</p><p><strong>Case presentation: </strong>Herein, we present a Persian male adult who manifested with epigastric pain, weakness, and a history of pleuritic chest pain two months prior to admission. The findings of the physical examination included vital signs within the normal range, unilateral fine crackle in the lung, abdominal distension with positive shifting dullness, and fluid wave test. Analysis of the ascitic fluid revealed a Serum-ascites albumin gradient (SAAG) of less than 1.1g/dl, indicating a non-portal condition. The results of the acid-fast bacilli (AFB) staining as well as the TB polymerase chain reaction (PCR) test were negative. However, the adenosine deaminase (ADA) level was 44 IU/L. A chest CT scan revealed mediastinal lymph node enlargement and pleural thickening with loculated pleural effusion. Three acid-fast bacilli smear of morning sputum were sent, and all three were negative. An abdominopelvic CT scan showed multiple periaortic and mesenteric lymph nodes of varying sizes with mesenteric haziness and accumulation of effusion in the peritoneal cavity. Eventually, peritoneal biopsy, the gold standard, was performed, which revealed multiple granulomatous lesions and areas of caseous necrosis surrounded by Langerhans giant cells and epithelioid cells.</p><p><strong>Conclusion: </strong>It is worth noting that in cases of ascites and pleural thickening, especially in patients with poor socioeconomic status, simultaneous pleural and peritoneal TB should be considered, especially in third-world countries.</p>","PeriodicalId":9646,"journal":{"name":"Caspian Journal of Internal Medicine","volume":"15 4","pages":"735-742"},"PeriodicalIF":1.0000,"publicationDate":"2024-09-07","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444099/pdf/","citationCount":"0","resultStr":"{\"title\":\"Concurrent peritoneal and pleural tuberculosis in an adult: A case report and literature review.\",\"authors\":\"Elham Barahimi, Zahra Ghaeini Hesarooeyeh, Ayoub Basham, Mohadeseh Karimi, Behnoush Heidari\",\"doi\":\"10.22088/cjim.15.4.735\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The simultaneous involvement of the pleura and peritoneum with tuberculosis in the absence of pulmonary foci is an uncommon condition that may lead physicians to misdiagnose.</p><p><strong>Case presentation: </strong>Herein, we present a Persian male adult who manifested with epigastric pain, weakness, and a history of pleuritic chest pain two months prior to admission. The findings of the physical examination included vital signs within the normal range, unilateral fine crackle in the lung, abdominal distension with positive shifting dullness, and fluid wave test. Analysis of the ascitic fluid revealed a Serum-ascites albumin gradient (SAAG) of less than 1.1g/dl, indicating a non-portal condition. The results of the acid-fast bacilli (AFB) staining as well as the TB polymerase chain reaction (PCR) test were negative. However, the adenosine deaminase (ADA) level was 44 IU/L. A chest CT scan revealed mediastinal lymph node enlargement and pleural thickening with loculated pleural effusion. Three acid-fast bacilli smear of morning sputum were sent, and all three were negative. An abdominopelvic CT scan showed multiple periaortic and mesenteric lymph nodes of varying sizes with mesenteric haziness and accumulation of effusion in the peritoneal cavity. Eventually, peritoneal biopsy, the gold standard, was performed, which revealed multiple granulomatous lesions and areas of caseous necrosis surrounded by Langerhans giant cells and epithelioid cells.</p><p><strong>Conclusion: </strong>It is worth noting that in cases of ascites and pleural thickening, especially in patients with poor socioeconomic status, simultaneous pleural and peritoneal TB should be considered, especially in third-world countries.</p>\",\"PeriodicalId\":9646,\"journal\":{\"name\":\"Caspian Journal of Internal Medicine\",\"volume\":\"15 4\",\"pages\":\"735-742\"},\"PeriodicalIF\":1.0000,\"publicationDate\":\"2024-09-07\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11444099/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Caspian Journal of Internal Medicine\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.22088/cjim.15.4.735\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Caspian Journal of Internal Medicine","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.22088/cjim.15.4.735","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Concurrent peritoneal and pleural tuberculosis in an adult: A case report and literature review.
Background: The simultaneous involvement of the pleura and peritoneum with tuberculosis in the absence of pulmonary foci is an uncommon condition that may lead physicians to misdiagnose.
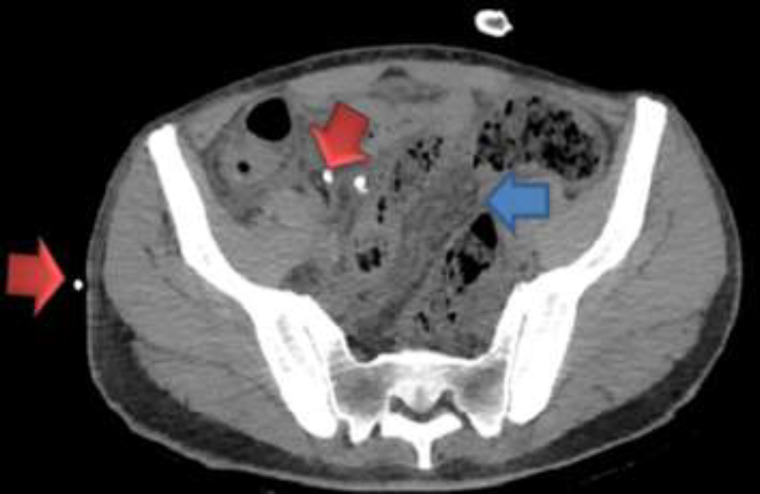
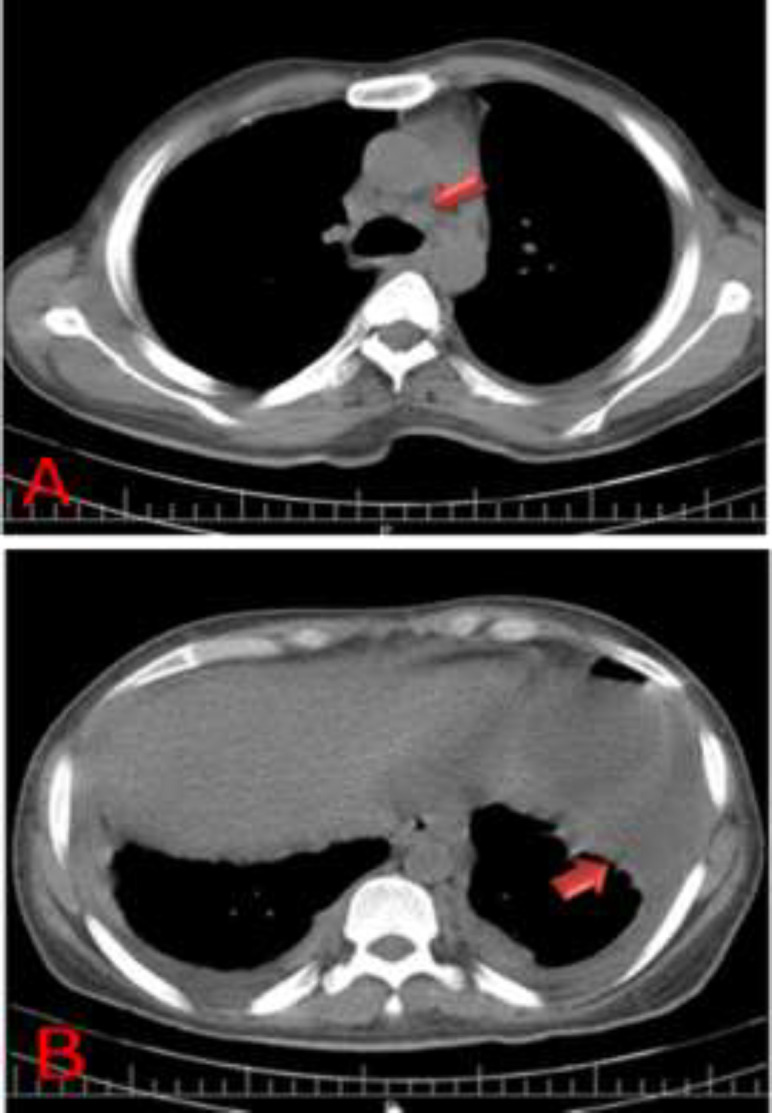
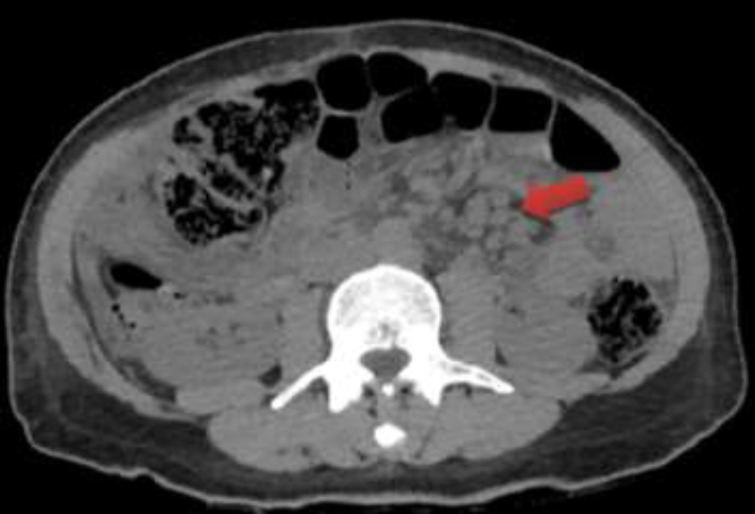
Case presentation: Herein, we present a Persian male adult who manifested with epigastric pain, weakness, and a history of pleuritic chest pain two months prior to admission. The findings of the physical examination included vital signs within the normal range, unilateral fine crackle in the lung, abdominal distension with positive shifting dullness, and fluid wave test. Analysis of the ascitic fluid revealed a Serum-ascites albumin gradient (SAAG) of less than 1.1g/dl, indicating a non-portal condition. The results of the acid-fast bacilli (AFB) staining as well as the TB polymerase chain reaction (PCR) test were negative. However, the adenosine deaminase (ADA) level was 44 IU/L. A chest CT scan revealed mediastinal lymph node enlargement and pleural thickening with loculated pleural effusion. Three acid-fast bacilli smear of morning sputum were sent, and all three were negative. An abdominopelvic CT scan showed multiple periaortic and mesenteric lymph nodes of varying sizes with mesenteric haziness and accumulation of effusion in the peritoneal cavity. Eventually, peritoneal biopsy, the gold standard, was performed, which revealed multiple granulomatous lesions and areas of caseous necrosis surrounded by Langerhans giant cells and epithelioid cells.
Conclusion: It is worth noting that in cases of ascites and pleural thickening, especially in patients with poor socioeconomic status, simultaneous pleural and peritoneal TB should be considered, especially in third-world countries.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


