Hyunki Park, Haeyoung Kim, Won Park, Won Kyung Cho, Nalee Kim, Tae Gyu Kim, Young-Hyuck Im, Jin Seok Ahn, Yeon Hee Park, Ji-Yeon Kim, Seok Jin Nam, Seok Won Kim, Jeong Eon Lee, Jonghan Yu, Byung Joo Chae, Sei Kyung Lee, Jai-Min Ryu
{"title":"术前化疗后三阴性乳腺癌残留患者的肿瘤治疗效果。","authors":"Hyunki Park, Haeyoung Kim, Won Park, Won Kyung Cho, Nalee Kim, Tae Gyu Kim, Young-Hyuck Im, Jin Seok Ahn, Yeon Hee Park, Ji-Yeon Kim, Seok Jin Nam, Seok Won Kim, Jeong Eon Lee, Jonghan Yu, Byung Joo Chae, Sei Kyung Lee, Jai-Min Ryu","doi":"10.3857/roj.2024.00087","DOIUrl":null,"url":null,"abstract":"<p><strong>Purpose: </strong>This study aimed to evaluate the clinical outcomes and prognostic implications of regional nodal irradiation (RNI) after neoadjuvant chemotherapy (NAC) in patients with residual triple-negative breast cancer (TNBC).</p><p><strong>Materials and methods: </strong>We analyzed 152 patients with residual TNBC who underwent breast-conserving surgery after NAC between December 2008 and December 2017. Most patients (n = 133; 87.5%) received taxane-based chemotherapy. Adjuvant radiotherapy (RT) was administered at a total dose of 45-65 Gy in 15-30 fractions to the whole breast, with some patients also receiving RT to regional nodes. Survival was calculated using the Kaplan-Meier method, and prognostic factors influencing survival were analyzed using the Cox proportional-hazards model.</p><p><strong>Results: </strong>During a median follow-up of 66 months (range, 9 to 179 months), the 5-year disease-free survival (DFS) rate was 68.0%. The 5-year locoregional recurrence-free survival, distant metastasis-free survival, and overall survival rates were 83.6%, 72.6%, and 78.7%, respectively. In the univariate analysis, the cN stage, ypT stage, ypN stage, axillary operation type, and RT field were associated with DFS. Multivariate analysis revealed that higher ypT stage (hazard ratio [HR] = 2.0; 95% confidence interval [CI] 1.00-3.82; p = 0.049) and ypN stage (HR = 4.7; 95% CI 1.57-14.24; p = 0.006) were associated with inferior DFS. Among clinically node-positive patients, those who received RT to the breast only had a 5-year DFS of 73.7%, whereas those who received RNI achieved a DFS of 59.6% (p = 0.164). There were no differences between the DFS and RNI.</p><p><strong>Conclusion: </strong>In patients with residual TNBC, higher ypT and ypN stages were associated with poorer outcomes after NAC. RNI did not appear to improve DFS. More intensive treatments incorporating systemic therapy and RT should be considered for these patients.</p>","PeriodicalId":94184,"journal":{"name":"Radiation oncology journal","volume":"42 3","pages":"210-217"},"PeriodicalIF":0.0000,"publicationDate":"2024-09-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467479/pdf/","citationCount":"0","resultStr":"{\"title\":\"Oncological outcomes in patients with residual triple-negative breast cancer after preoperative chemotherapy.\",\"authors\":\"Hyunki Park, Haeyoung Kim, Won Park, Won Kyung Cho, Nalee Kim, Tae Gyu Kim, Young-Hyuck Im, Jin Seok Ahn, Yeon Hee Park, Ji-Yeon Kim, Seok Jin Nam, Seok Won Kim, Jeong Eon Lee, Jonghan Yu, Byung Joo Chae, Sei Kyung Lee, Jai-Min Ryu\",\"doi\":\"10.3857/roj.2024.00087\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Purpose: </strong>This study aimed to evaluate the clinical outcomes and prognostic implications of regional nodal irradiation (RNI) after neoadjuvant chemotherapy (NAC) in patients with residual triple-negative breast cancer (TNBC).</p><p><strong>Materials and methods: </strong>We analyzed 152 patients with residual TNBC who underwent breast-conserving surgery after NAC between December 2008 and December 2017. Most patients (n = 133; 87.5%) received taxane-based chemotherapy. Adjuvant radiotherapy (RT) was administered at a total dose of 45-65 Gy in 15-30 fractions to the whole breast, with some patients also receiving RT to regional nodes. Survival was calculated using the Kaplan-Meier method, and prognostic factors influencing survival were analyzed using the Cox proportional-hazards model.</p><p><strong>Results: </strong>During a median follow-up of 66 months (range, 9 to 179 months), the 5-year disease-free survival (DFS) rate was 68.0%. The 5-year locoregional recurrence-free survival, distant metastasis-free survival, and overall survival rates were 83.6%, 72.6%, and 78.7%, respectively. In the univariate analysis, the cN stage, ypT stage, ypN stage, axillary operation type, and RT field were associated with DFS. Multivariate analysis revealed that higher ypT stage (hazard ratio [HR] = 2.0; 95% confidence interval [CI] 1.00-3.82; p = 0.049) and ypN stage (HR = 4.7; 95% CI 1.57-14.24; p = 0.006) were associated with inferior DFS. Among clinically node-positive patients, those who received RT to the breast only had a 5-year DFS of 73.7%, whereas those who received RNI achieved a DFS of 59.6% (p = 0.164). There were no differences between the DFS and RNI.</p><p><strong>Conclusion: </strong>In patients with residual TNBC, higher ypT and ypN stages were associated with poorer outcomes after NAC. RNI did not appear to improve DFS. More intensive treatments incorporating systemic therapy and RT should be considered for these patients.</p>\",\"PeriodicalId\":94184,\"journal\":{\"name\":\"Radiation oncology journal\",\"volume\":\"42 3\",\"pages\":\"210-217\"},\"PeriodicalIF\":0.0000,\"publicationDate\":\"2024-09-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11467479/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Radiation oncology journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.3857/roj.2024.00087\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/20 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"\",\"JCRName\":\"\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Radiation oncology journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.3857/roj.2024.00087","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/20 0:00:00","PubModel":"Epub","JCR":"","JCRName":"","Score":null,"Total":0}
Oncological outcomes in patients with residual triple-negative breast cancer after preoperative chemotherapy.
Purpose: This study aimed to evaluate the clinical outcomes and prognostic implications of regional nodal irradiation (RNI) after neoadjuvant chemotherapy (NAC) in patients with residual triple-negative breast cancer (TNBC).
Materials and methods: We analyzed 152 patients with residual TNBC who underwent breast-conserving surgery after NAC between December 2008 and December 2017. Most patients (n = 133; 87.5%) received taxane-based chemotherapy. Adjuvant radiotherapy (RT) was administered at a total dose of 45-65 Gy in 15-30 fractions to the whole breast, with some patients also receiving RT to regional nodes. Survival was calculated using the Kaplan-Meier method, and prognostic factors influencing survival were analyzed using the Cox proportional-hazards model.
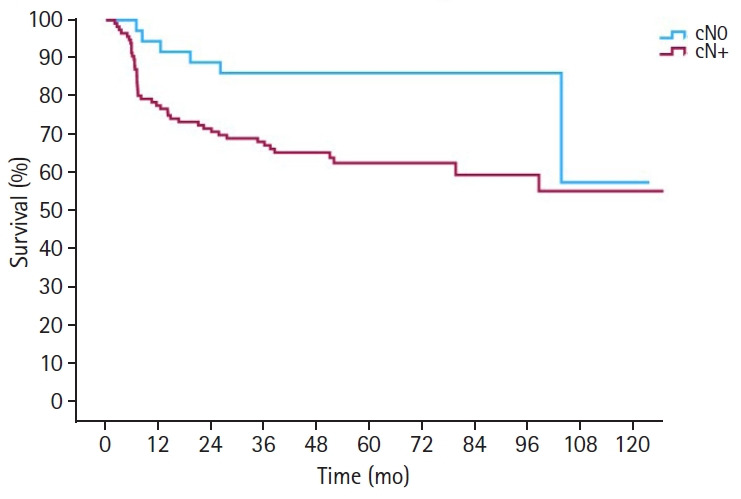
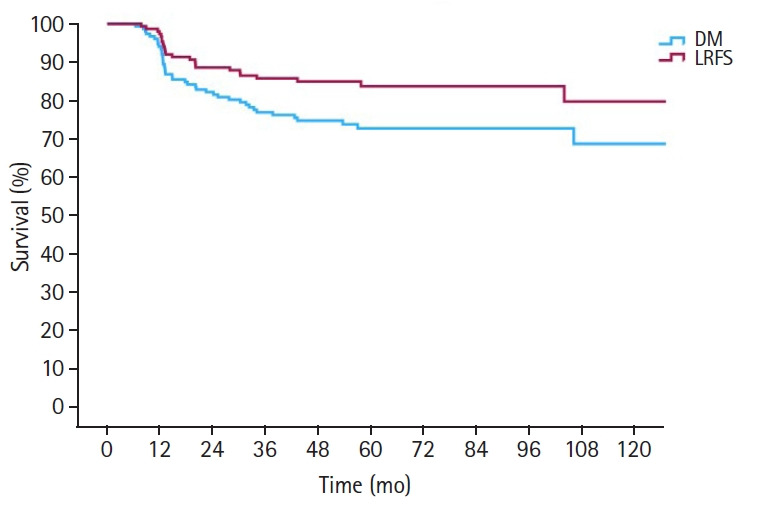
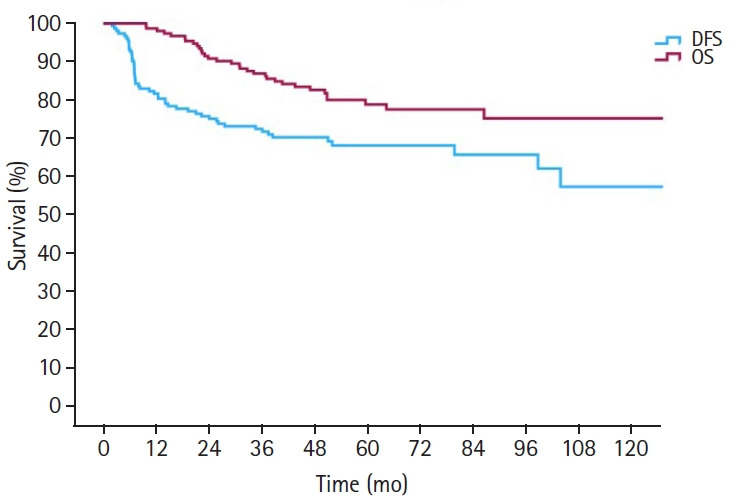
Results: During a median follow-up of 66 months (range, 9 to 179 months), the 5-year disease-free survival (DFS) rate was 68.0%. The 5-year locoregional recurrence-free survival, distant metastasis-free survival, and overall survival rates were 83.6%, 72.6%, and 78.7%, respectively. In the univariate analysis, the cN stage, ypT stage, ypN stage, axillary operation type, and RT field were associated with DFS. Multivariate analysis revealed that higher ypT stage (hazard ratio [HR] = 2.0; 95% confidence interval [CI] 1.00-3.82; p = 0.049) and ypN stage (HR = 4.7; 95% CI 1.57-14.24; p = 0.006) were associated with inferior DFS. Among clinically node-positive patients, those who received RT to the breast only had a 5-year DFS of 73.7%, whereas those who received RNI achieved a DFS of 59.6% (p = 0.164). There were no differences between the DFS and RNI.
Conclusion: In patients with residual TNBC, higher ypT and ypN stages were associated with poorer outcomes after NAC. RNI did not appear to improve DFS. More intensive treatments incorporating systemic therapy and RT should be considered for these patients.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


