K R Surag, Abhijit Shah, Kasi Vishwanath Gali, A V B Krishnakanth, Arun Chawla, Padmaraj Hegde, Anupam Choudhary, Mithun Rao
{"title":"无管 \"经皮肾镜碎石术后患者严重出血:血管栓塞的预测因素。","authors":"K R Surag, Abhijit Shah, Kasi Vishwanath Gali, A V B Krishnakanth, Arun Chawla, Padmaraj Hegde, Anupam Choudhary, Mithun Rao","doi":"10.1177/03915603241282409","DOIUrl":null,"url":null,"abstract":"<p><strong>Introduction: </strong>Percutaneous nephrolithotomy (PCNL) is a widely used procedure for treating renal calculi. Advanced techniques have improved outcomes, but hemorrhage remains a significant complication. While most cases of hemorrhagic complications are typically managed conservatively, few cases necessitate interventions like angioembolization (AE). The purpose of this study is to identify risk factors closely associated with severe bleeding post-PCNL requiring AE and to assess if these factors can independently predict the type of lesion [arteriovenous fistula (AVF) vs pseudoaneurysm (PA)].</p><p><strong>Materials and method: </strong>A retrospective analysis was conducted on 119 patients who underwent \"tubeless\" PCNL and experienced severe bleeding between January 2018 and December 2023. The study reviewed demographic characteristics, stone characteristics, perioperative factors, and adverse events. The chi-square test and Fisher's exact test were used for univariate analysis. Logistic regression analysis was used in binomial analysis with a value of <i>p</i> < 0.05 considered statistically significant.</p><p><strong>Results: </strong>Out of 119 patients, 51 required AE. Elevated preoperative serum creatinine levels (>1.5 mg/dl) [<i>p</i> = 0.01], upper pole access [<i>p</i> = 0.008], and a larger access sheath size (standard PCNL vs mini-PCNL) [<i>p</i> ⩽ 0.001] were found to be significantly associated with AE. Logistic regression analysis revealed standard PCNL was significantly associated with post-PCNL bleeding requiring AE (odds ratio [OR]: 50, 95% confidence interval [CI]: 6.529-382.90, <i>p</i> ⩽ 0.001). Stone size and co-morbidities showed no significant association with AE. The average duration of presentation of symptoms post PCNL was 13.6 days. Most patients underwent coiling for AE, with a clinical success rate of 94%.</p><p><strong>Conclusion: </strong>Elevated serum creatinine levels, upper pole access, and tract size >24 Fr are more prone to post-tubeless PCNL severe bleeding, which requires renal AE. The findings suggest that early angiography and possible AE should be considered for at-risk patients. In the future, these predictors may be integrated into predictive models to improve patient risk stratification.</p>","PeriodicalId":23574,"journal":{"name":"Urologia Journal","volume":" ","pages":"89-95"},"PeriodicalIF":0.7000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11806643/pdf/","citationCount":"0","resultStr":"{\"title\":\"Severe bleeding in patients following \\\"tubeless\\\" percutaneous nephrolithotomy: Predictors of angioembolization.\",\"authors\":\"K R Surag, Abhijit Shah, Kasi Vishwanath Gali, A V B Krishnakanth, Arun Chawla, Padmaraj Hegde, Anupam Choudhary, Mithun Rao\",\"doi\":\"10.1177/03915603241282409\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Introduction: </strong>Percutaneous nephrolithotomy (PCNL) is a widely used procedure for treating renal calculi. Advanced techniques have improved outcomes, but hemorrhage remains a significant complication. While most cases of hemorrhagic complications are typically managed conservatively, few cases necessitate interventions like angioembolization (AE). The purpose of this study is to identify risk factors closely associated with severe bleeding post-PCNL requiring AE and to assess if these factors can independently predict the type of lesion [arteriovenous fistula (AVF) vs pseudoaneurysm (PA)].</p><p><strong>Materials and method: </strong>A retrospective analysis was conducted on 119 patients who underwent \\\"tubeless\\\" PCNL and experienced severe bleeding between January 2018 and December 2023. The study reviewed demographic characteristics, stone characteristics, perioperative factors, and adverse events. The chi-square test and Fisher's exact test were used for univariate analysis. Logistic regression analysis was used in binomial analysis with a value of <i>p</i> < 0.05 considered statistically significant.</p><p><strong>Results: </strong>Out of 119 patients, 51 required AE. Elevated preoperative serum creatinine levels (>1.5 mg/dl) [<i>p</i> = 0.01], upper pole access [<i>p</i> = 0.008], and a larger access sheath size (standard PCNL vs mini-PCNL) [<i>p</i> ⩽ 0.001] were found to be significantly associated with AE. Logistic regression analysis revealed standard PCNL was significantly associated with post-PCNL bleeding requiring AE (odds ratio [OR]: 50, 95% confidence interval [CI]: 6.529-382.90, <i>p</i> ⩽ 0.001). Stone size and co-morbidities showed no significant association with AE. The average duration of presentation of symptoms post PCNL was 13.6 days. Most patients underwent coiling for AE, with a clinical success rate of 94%.</p><p><strong>Conclusion: </strong>Elevated serum creatinine levels, upper pole access, and tract size >24 Fr are more prone to post-tubeless PCNL severe bleeding, which requires renal AE. The findings suggest that early angiography and possible AE should be considered for at-risk patients. In the future, these predictors may be integrated into predictive models to improve patient risk stratification.</p>\",\"PeriodicalId\":23574,\"journal\":{\"name\":\"Urologia Journal\",\"volume\":\" \",\"pages\":\"89-95\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11806643/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Urologia Journal\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/03915603241282409\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/30 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q4\",\"JCRName\":\"UROLOGY & NEPHROLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Urologia Journal","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/03915603241282409","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/30 0:00:00","PubModel":"Epub","JCR":"Q4","JCRName":"UROLOGY & NEPHROLOGY","Score":null,"Total":0}
Severe bleeding in patients following "tubeless" percutaneous nephrolithotomy: Predictors of angioembolization.
Introduction: Percutaneous nephrolithotomy (PCNL) is a widely used procedure for treating renal calculi. Advanced techniques have improved outcomes, but hemorrhage remains a significant complication. While most cases of hemorrhagic complications are typically managed conservatively, few cases necessitate interventions like angioembolization (AE). The purpose of this study is to identify risk factors closely associated with severe bleeding post-PCNL requiring AE and to assess if these factors can independently predict the type of lesion [arteriovenous fistula (AVF) vs pseudoaneurysm (PA)].
Materials and method: A retrospective analysis was conducted on 119 patients who underwent "tubeless" PCNL and experienced severe bleeding between January 2018 and December 2023. The study reviewed demographic characteristics, stone characteristics, perioperative factors, and adverse events. The chi-square test and Fisher's exact test were used for univariate analysis. Logistic regression analysis was used in binomial analysis with a value of p < 0.05 considered statistically significant.
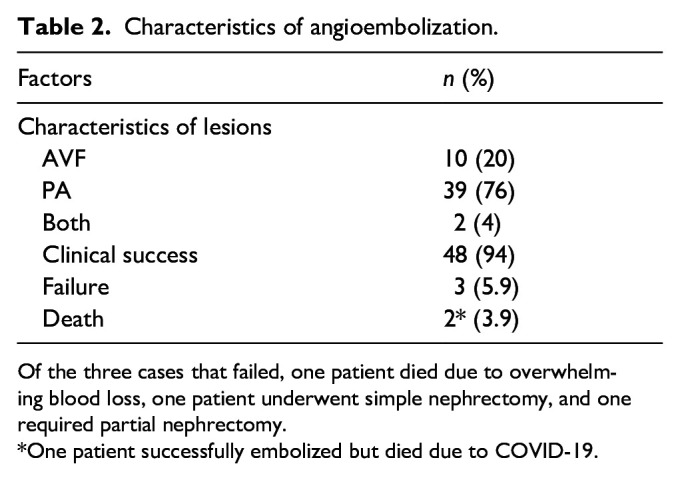
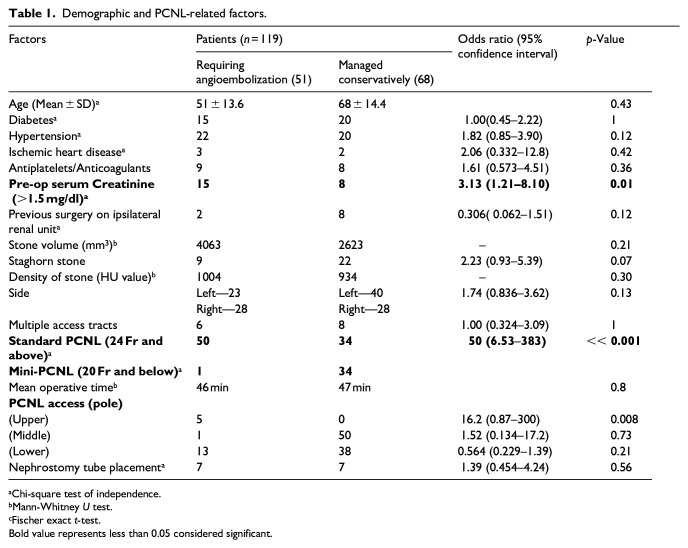
Results: Out of 119 patients, 51 required AE. Elevated preoperative serum creatinine levels (>1.5 mg/dl) [p = 0.01], upper pole access [p = 0.008], and a larger access sheath size (standard PCNL vs mini-PCNL) [p ⩽ 0.001] were found to be significantly associated with AE. Logistic regression analysis revealed standard PCNL was significantly associated with post-PCNL bleeding requiring AE (odds ratio [OR]: 50, 95% confidence interval [CI]: 6.529-382.90, p ⩽ 0.001). Stone size and co-morbidities showed no significant association with AE. The average duration of presentation of symptoms post PCNL was 13.6 days. Most patients underwent coiling for AE, with a clinical success rate of 94%.
Conclusion: Elevated serum creatinine levels, upper pole access, and tract size >24 Fr are more prone to post-tubeless PCNL severe bleeding, which requires renal AE. The findings suggest that early angiography and possible AE should be considered for at-risk patients. In the future, these predictors may be integrated into predictive models to improve patient risk stratification.


 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


