{"title":"水肿性腹水?严重甲状腺功能减退症腹水的罕见表现:病例报告与综述。","authors":"Kylie Divashnee Konar, Somasundram Pillay, Nishan Sookdev","doi":"10.1177/2050313X241282218","DOIUrl":null,"url":null,"abstract":"<p><p>Ascites represents an infrequent sequela of hypothyroidism, manifesting in fewer than 4% of affected individuals. Herein, we delineate a case characterized by profound hypothyroidism accompanied by substantial ascites, further complicated by cardiac insufficiency. A 29-year-old female, previously diagnosed with postradiation hypothyroidism subsequent to a diagnosis of Grave's disease 11 years prior, presented with exacerbating dyspnoea, abdominal distension, and orthopnea. In January 2024, she was admitted with massive ascites, exhibiting clinical manifestations of both hypothyroidism and cardiac failure. Thyroid function tests were markedly abnormal, with a thyroid-stimulating hormone level of 77.65 mIU/L, triiodothyronine at 2.2 nmol/L, and thyroxine levels below 3.2 pmol/L. Echocardiographic evaluation revealed dilated cardiomyopathy with a significantly reduced systolic (ejection fraction of 25.9%) and diastolic function (E/A ratio of 0.87). Analysis of the ascitic fluid demonstrated a serum-ascites albumin gradient exceeding 1.1 g/L (3 g/L). Ultrasonography of the abdomen ruled out portal hypertension, while computed tomography of the abdomen confirmed extensive ascites without evidence of malignancy. Under the supervision of a specialist, the patient was administered a high dosage of levothyroxine (300 mcg), leading to a significant amelioration in both thyroid function parameters and her ascites. Subsequent thyroid function tests demonstrated a decrease in thyroid-stimulating hormone levels to 11.7 mIU/L and an increase in thyroxine levels to 15.6 pmol/L, indicating a positive response to the thyroid hormone replacement therapy. Subsequent echocardiographic assessment showed improvement in the ejection fraction to 26.9% and diastolic function (E/A ratio of 1.27). Myxedema ascites, though infrequent, is readily amenable to treatment. The serum-ascites albumin gradient exceeding 1.1 g/L may be indicative of hypothyroidism-associated ascites, although the paucity of studies renders it uncertain whether this is a characteristic feature. Further investigation into the etiology, diagnostic criteria, and management strategies for ascites in the context of hypothyroidism is warranted.</p>","PeriodicalId":21418,"journal":{"name":"SAGE Open Medical Case Reports","volume":"12 ","pages":"2050313X241282218"},"PeriodicalIF":0.6000,"publicationDate":"2024-09-25","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11425730/pdf/","citationCount":"0","resultStr":"{\"title\":\"Myxedema ascites? A rare presentation of ascites in severe hypothyroidism: A case report and review.\",\"authors\":\"Kylie Divashnee Konar, Somasundram Pillay, Nishan Sookdev\",\"doi\":\"10.1177/2050313X241282218\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>Ascites represents an infrequent sequela of hypothyroidism, manifesting in fewer than 4% of affected individuals. Herein, we delineate a case characterized by profound hypothyroidism accompanied by substantial ascites, further complicated by cardiac insufficiency. A 29-year-old female, previously diagnosed with postradiation hypothyroidism subsequent to a diagnosis of Grave's disease 11 years prior, presented with exacerbating dyspnoea, abdominal distension, and orthopnea. In January 2024, she was admitted with massive ascites, exhibiting clinical manifestations of both hypothyroidism and cardiac failure. Thyroid function tests were markedly abnormal, with a thyroid-stimulating hormone level of 77.65 mIU/L, triiodothyronine at 2.2 nmol/L, and thyroxine levels below 3.2 pmol/L. Echocardiographic evaluation revealed dilated cardiomyopathy with a significantly reduced systolic (ejection fraction of 25.9%) and diastolic function (E/A ratio of 0.87). Analysis of the ascitic fluid demonstrated a serum-ascites albumin gradient exceeding 1.1 g/L (3 g/L). Ultrasonography of the abdomen ruled out portal hypertension, while computed tomography of the abdomen confirmed extensive ascites without evidence of malignancy. Under the supervision of a specialist, the patient was administered a high dosage of levothyroxine (300 mcg), leading to a significant amelioration in both thyroid function parameters and her ascites. Subsequent thyroid function tests demonstrated a decrease in thyroid-stimulating hormone levels to 11.7 mIU/L and an increase in thyroxine levels to 15.6 pmol/L, indicating a positive response to the thyroid hormone replacement therapy. Subsequent echocardiographic assessment showed improvement in the ejection fraction to 26.9% and diastolic function (E/A ratio of 1.27). Myxedema ascites, though infrequent, is readily amenable to treatment. The serum-ascites albumin gradient exceeding 1.1 g/L may be indicative of hypothyroidism-associated ascites, although the paucity of studies renders it uncertain whether this is a characteristic feature. Further investigation into the etiology, diagnostic criteria, and management strategies for ascites in the context of hypothyroidism is warranted.</p>\",\"PeriodicalId\":21418,\"journal\":{\"name\":\"SAGE Open Medical Case Reports\",\"volume\":\"12 \",\"pages\":\"2050313X241282218\"},\"PeriodicalIF\":0.6000,\"publicationDate\":\"2024-09-25\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11425730/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"SAGE Open Medical Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.1177/2050313X241282218\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/1/1 0:00:00\",\"PubModel\":\"eCollection\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"SAGE Open Medical Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.1177/2050313X241282218","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/1/1 0:00:00","PubModel":"eCollection","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
Myxedema ascites? A rare presentation of ascites in severe hypothyroidism: A case report and review.
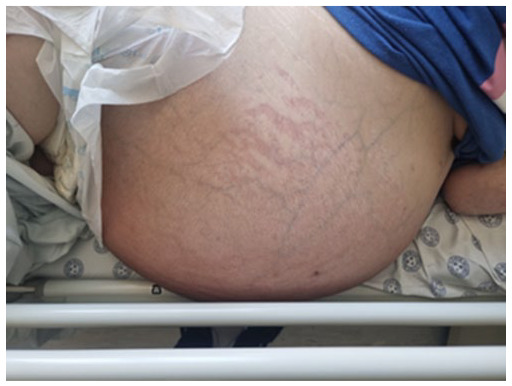
Ascites represents an infrequent sequela of hypothyroidism, manifesting in fewer than 4% of affected individuals. Herein, we delineate a case characterized by profound hypothyroidism accompanied by substantial ascites, further complicated by cardiac insufficiency. A 29-year-old female, previously diagnosed with postradiation hypothyroidism subsequent to a diagnosis of Grave's disease 11 years prior, presented with exacerbating dyspnoea, abdominal distension, and orthopnea. In January 2024, she was admitted with massive ascites, exhibiting clinical manifestations of both hypothyroidism and cardiac failure. Thyroid function tests were markedly abnormal, with a thyroid-stimulating hormone level of 77.65 mIU/L, triiodothyronine at 2.2 nmol/L, and thyroxine levels below 3.2 pmol/L. Echocardiographic evaluation revealed dilated cardiomyopathy with a significantly reduced systolic (ejection fraction of 25.9%) and diastolic function (E/A ratio of 0.87). Analysis of the ascitic fluid demonstrated a serum-ascites albumin gradient exceeding 1.1 g/L (3 g/L). Ultrasonography of the abdomen ruled out portal hypertension, while computed tomography of the abdomen confirmed extensive ascites without evidence of malignancy. Under the supervision of a specialist, the patient was administered a high dosage of levothyroxine (300 mcg), leading to a significant amelioration in both thyroid function parameters and her ascites. Subsequent thyroid function tests demonstrated a decrease in thyroid-stimulating hormone levels to 11.7 mIU/L and an increase in thyroxine levels to 15.6 pmol/L, indicating a positive response to the thyroid hormone replacement therapy. Subsequent echocardiographic assessment showed improvement in the ejection fraction to 26.9% and diastolic function (E/A ratio of 1.27). Myxedema ascites, though infrequent, is readily amenable to treatment. The serum-ascites albumin gradient exceeding 1.1 g/L may be indicative of hypothyroidism-associated ascites, although the paucity of studies renders it uncertain whether this is a characteristic feature. Further investigation into the etiology, diagnostic criteria, and management strategies for ascites in the context of hypothyroidism is warranted.
期刊介绍:
SAGE Open Medical Case Reports (indexed in PubMed Central) is a peer reviewed, open access journal. It aims to provide a publication home for short case reports and case series, which often do not find a place in traditional primary research journals, but provide key insights into real medical cases that are essential for physicians, and may ultimately help to improve patient outcomes. SAGE Open Medical Case Reports does not limit content due to page budgets or thematic significance. Papers are subject to rigorous peer review and are selected on the basis of whether the research is sound and deserves publication. By virtue of not restricting papers to a narrow discipline, SAGE Open Medical Case Reports facilitates the discovery of the connections between papers, whether within or between disciplines. Case reports can span the full spectrum of medicine across the health sciences in the broadest sense, including: Allergy/Immunology Anaesthesia/Pain Cardiovascular Critical Care/ Emergency Medicine Dentistry Dermatology Diabetes/Endocrinology Epidemiology/Public Health Gastroenterology/Hepatology Geriatrics/Gerontology Haematology Infectious Diseases Mental Health/Psychiatry Nephrology Neurology Nursing Obstetrics/Gynaecology Oncology Ophthalmology Orthopaedics/Rehabilitation/Occupational Therapy Otolaryngology Palliative Medicine Pathology Pharmacoeconomics/health economics Pharmacoepidemiology/Drug safety Psychopharmacology Radiology Respiratory Medicine Rheumatology/ Clinical Immunology Sports Medicine Surgery Toxicology Urology Women''s Health.



 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


