Jaewon Jang, Hye Jin Kim, Hyun Joo Kim, Wyun Kon Park
{"title":"使用改良的 Rapid-O2 氧气充气装置进行经导管通气。","authors":"Jaewon Jang, Hye Jin Kim, Hyun Joo Kim, Wyun Kon Park","doi":"10.4097/kja.24095","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>The Rapid-O2 oxygen insufflation device® (Rapid-O2) was designed primarily for rescue oxygenation in cannot intubate, cannot oxygenate (CICO) events; thus, hypercapnia is inevitable. Rapid-O2 was modified to enhance ventilation using the Venturi effect during expiration.</p><p><strong>Methods: </strong>To determine the most effective combination of inner catheters (20 gauge [G], 18 G, 16 G, 14 G, and 2-mm inner diameter [ID] transtracheal catheter [TTC]) and insufflation catheters (16 G, 14 G, and 2-mm ID TTC) for achieving optimum ventilation, insufflating and expiratory flows were measured at an oxygen flow rate of 15 L/min. The insufflating and expiratory pressures were measured at 6-15 L/min. The flows and pressures were measured using a gas flow analyzer. The insufflating and expiratory times were measured using a trachea-lung model to obtain minute volumes. To assess the improvement by modifying the Rapid-O2, minute volumes were measured using the Rapid-O2.</p><p><strong>Results: </strong>The most appropriate inner catheter was 18 G. The insufflating pressures ranged from 97 (2-mm ID TTC) to 377 cmH2O (16 G) at 15 L/min. During expiration, similar negative pressures of 50 cmH2O were measured in the insufflation catheters at 15 L/min. At lung compliance of 100 ml/cmH2O, the minute volumes through a 2-mm ID and 14 G insufflation catheters were 7.0 and 5.37 L/min, respectively, at 15 L/min. The minute volumes were significantly greater in modified Rapid-O2.</p><p><strong>Conclusions: </strong>Modified Rapid-O2 provided sufficient minute volumes in adults using a 14 G or 2-mm ID insufflation catheter at 15 L/min, demonstrating its potential for ventilation in CICO events.</p>","PeriodicalId":17855,"journal":{"name":"Korean Journal of Anesthesiology","volume":" ","pages":"61-72"},"PeriodicalIF":6.3000,"publicationDate":"2025-02-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11836609/pdf/","citationCount":"0","resultStr":"{\"title\":\"Transcatheter ventilation with a modified Rapid-O2 oxygen insufflation device.\",\"authors\":\"Jaewon Jang, Hye Jin Kim, Hyun Joo Kim, Wyun Kon Park\",\"doi\":\"10.4097/kja.24095\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>The Rapid-O2 oxygen insufflation device® (Rapid-O2) was designed primarily for rescue oxygenation in cannot intubate, cannot oxygenate (CICO) events; thus, hypercapnia is inevitable. Rapid-O2 was modified to enhance ventilation using the Venturi effect during expiration.</p><p><strong>Methods: </strong>To determine the most effective combination of inner catheters (20 gauge [G], 18 G, 16 G, 14 G, and 2-mm inner diameter [ID] transtracheal catheter [TTC]) and insufflation catheters (16 G, 14 G, and 2-mm ID TTC) for achieving optimum ventilation, insufflating and expiratory flows were measured at an oxygen flow rate of 15 L/min. The insufflating and expiratory pressures were measured at 6-15 L/min. The flows and pressures were measured using a gas flow analyzer. The insufflating and expiratory times were measured using a trachea-lung model to obtain minute volumes. To assess the improvement by modifying the Rapid-O2, minute volumes were measured using the Rapid-O2.</p><p><strong>Results: </strong>The most appropriate inner catheter was 18 G. The insufflating pressures ranged from 97 (2-mm ID TTC) to 377 cmH2O (16 G) at 15 L/min. During expiration, similar negative pressures of 50 cmH2O were measured in the insufflation catheters at 15 L/min. At lung compliance of 100 ml/cmH2O, the minute volumes through a 2-mm ID and 14 G insufflation catheters were 7.0 and 5.37 L/min, respectively, at 15 L/min. The minute volumes were significantly greater in modified Rapid-O2.</p><p><strong>Conclusions: </strong>Modified Rapid-O2 provided sufficient minute volumes in adults using a 14 G or 2-mm ID insufflation catheter at 15 L/min, demonstrating its potential for ventilation in CICO events.</p>\",\"PeriodicalId\":17855,\"journal\":{\"name\":\"Korean Journal of Anesthesiology\",\"volume\":\" \",\"pages\":\"61-72\"},\"PeriodicalIF\":6.3000,\"publicationDate\":\"2025-02-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11836609/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Korean Journal of Anesthesiology\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.4097/kja.24095\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"2024/9/27 0:00:00\",\"PubModel\":\"Epub\",\"JCR\":\"Q1\",\"JCRName\":\"ANESTHESIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Korean Journal of Anesthesiology","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.4097/kja.24095","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"2024/9/27 0:00:00","PubModel":"Epub","JCR":"Q1","JCRName":"ANESTHESIOLOGY","Score":null,"Total":0}
Transcatheter ventilation with a modified Rapid-O2 oxygen insufflation device.
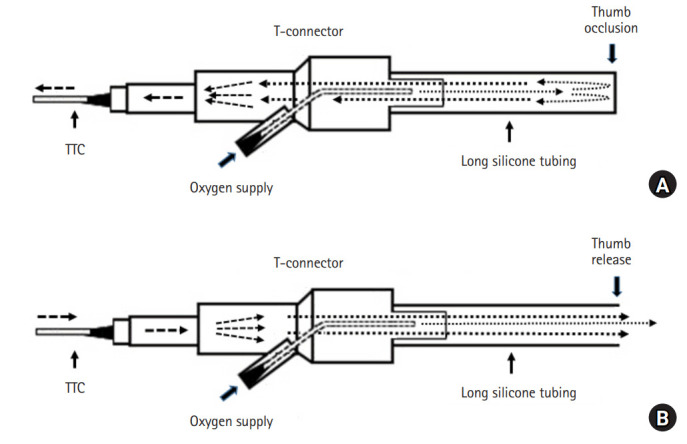
Background: The Rapid-O2 oxygen insufflation device® (Rapid-O2) was designed primarily for rescue oxygenation in cannot intubate, cannot oxygenate (CICO) events; thus, hypercapnia is inevitable. Rapid-O2 was modified to enhance ventilation using the Venturi effect during expiration.
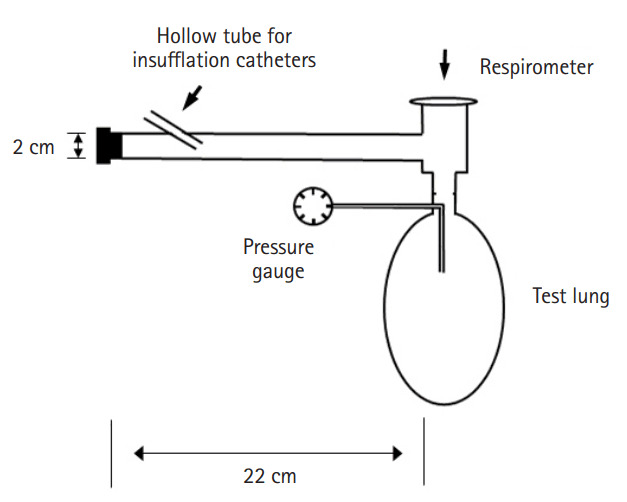
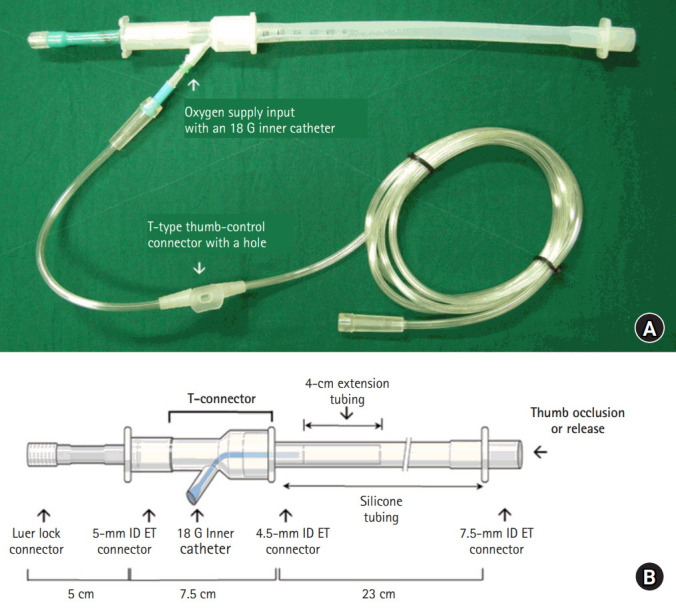
Methods: To determine the most effective combination of inner catheters (20 gauge [G], 18 G, 16 G, 14 G, and 2-mm inner diameter [ID] transtracheal catheter [TTC]) and insufflation catheters (16 G, 14 G, and 2-mm ID TTC) for achieving optimum ventilation, insufflating and expiratory flows were measured at an oxygen flow rate of 15 L/min. The insufflating and expiratory pressures were measured at 6-15 L/min. The flows and pressures were measured using a gas flow analyzer. The insufflating and expiratory times were measured using a trachea-lung model to obtain minute volumes. To assess the improvement by modifying the Rapid-O2, minute volumes were measured using the Rapid-O2.
Results: The most appropriate inner catheter was 18 G. The insufflating pressures ranged from 97 (2-mm ID TTC) to 377 cmH2O (16 G) at 15 L/min. During expiration, similar negative pressures of 50 cmH2O were measured in the insufflation catheters at 15 L/min. At lung compliance of 100 ml/cmH2O, the minute volumes through a 2-mm ID and 14 G insufflation catheters were 7.0 and 5.37 L/min, respectively, at 15 L/min. The minute volumes were significantly greater in modified Rapid-O2.
Conclusions: Modified Rapid-O2 provided sufficient minute volumes in adults using a 14 G or 2-mm ID insufflation catheter at 15 L/min, demonstrating its potential for ventilation in CICO events.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


