Sofia Hemrage, Stephen Parkin, Nicola Kalk, Naina Shah, Paolo Deluca, Colin Drummond
{"title":"以代金券为基础的应急管理,促进合并酒精使用障碍和酒精相关肝病患者参与治疗:以服务使用者为对象的试点理论定性研究。","authors":"Sofia Hemrage, Stephen Parkin, Nicola Kalk, Naina Shah, Paolo Deluca, Colin Drummond","doi":"10.1111/acer.15450","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Background</h3>\n \n <p>Effective interventions for the management of alcohol-related liver disease (ARLD) remain a gap in clinical practice, and patients' engagement with alcohol services is suboptimal. Based upon the principles of operant conditioning, contingency management (CM) is a psychosocial intervention th\tat involves gradual, increasing incentives upon completion of treatment-related goals such as treatment attendance.</p>\n </section>\n \n <section>\n \n <h3> Methods</h3>\n \n <p>A pilot feasibility trial was conducted with 30 adult patients recruited from an inpatient clinical setting. Consecutive sampling was used to recruit patients presenting comorbid alcohol use disorder (AUD) and ARLD. Participants were randomized to integrated liver care (ILC), receiving hepatology and AUD care, or ILC with a voucher-based CM intervention (intervention arm). A longitudinal qualitative approach was adopted to explore anticipated (Stage 1) and experienced acceptability (Stage 2). The Theoretical Framework of Acceptability (TFA) guided semi-structured in-depth interviews and deductive analysis.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Thirty participants were enrolled in the pilot trial, and interviews were conducted with 24 participants at Stage 1 and seven at Stage 2. Over half of the cohort (54.2%, <i>n</i> = 13) presented decompensated liver disease, and an average of 179 units of alcohol were consumed per week. Overall positive views toward voucher-based CM were noted, and explanatory data emerged across five TFA domains (<i>intervention coherence</i>, <i>ethicality, self-efficacy, perceived effectiveness, and affective attitude</i>). The core aspects of the voucher-based CM intervention matched participants' preferences and needs. Participants regarded CM as having a symbolic value and strengthening the therapeutic alliance with healthcare providers.</p>\n </section>\n \n <section>\n \n <h3> Conclusion</h3>\n \n <p>The data support the scope of voucher-based CM intervention to promote engagement with treatment services, and its potential to address the gaps in the care continuum in ARLD. The findings are of practical significance for developing person-centered, tailored interventions for this clinical population. The outcomes of this investigation can inform decision-making among stakeholders and healthcare providers and improve health outcomes for this clinical population.</p>\n </section>\n </div>","PeriodicalId":72145,"journal":{"name":"Alcohol (Hanover, York County, Pa.)","volume":"48 11","pages":"2160-2174"},"PeriodicalIF":2.7000,"publicationDate":"2024-09-26","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/acer.15450","citationCount":"0","resultStr":"{\"title\":\"Voucher-based contingency management to promote treatment engagement in comorbid alcohol use disorder and alcohol-related liver disease: A pilot theory-informed qualitative study with service users\",\"authors\":\"Sofia Hemrage, Stephen Parkin, Nicola Kalk, Naina Shah, Paolo Deluca, Colin Drummond\",\"doi\":\"10.1111/acer.15450\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Background</h3>\\n \\n <p>Effective interventions for the management of alcohol-related liver disease (ARLD) remain a gap in clinical practice, and patients' engagement with alcohol services is suboptimal. Based upon the principles of operant conditioning, contingency management (CM) is a psychosocial intervention th\\tat involves gradual, increasing incentives upon completion of treatment-related goals such as treatment attendance.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Methods</h3>\\n \\n <p>A pilot feasibility trial was conducted with 30 adult patients recruited from an inpatient clinical setting. Consecutive sampling was used to recruit patients presenting comorbid alcohol use disorder (AUD) and ARLD. Participants were randomized to integrated liver care (ILC), receiving hepatology and AUD care, or ILC with a voucher-based CM intervention (intervention arm). A longitudinal qualitative approach was adopted to explore anticipated (Stage 1) and experienced acceptability (Stage 2). The Theoretical Framework of Acceptability (TFA) guided semi-structured in-depth interviews and deductive analysis.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Thirty participants were enrolled in the pilot trial, and interviews were conducted with 24 participants at Stage 1 and seven at Stage 2. Over half of the cohort (54.2%, <i>n</i> = 13) presented decompensated liver disease, and an average of 179 units of alcohol were consumed per week. Overall positive views toward voucher-based CM were noted, and explanatory data emerged across five TFA domains (<i>intervention coherence</i>, <i>ethicality, self-efficacy, perceived effectiveness, and affective attitude</i>). The core aspects of the voucher-based CM intervention matched participants' preferences and needs. Participants regarded CM as having a symbolic value and strengthening the therapeutic alliance with healthcare providers.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusion</h3>\\n \\n <p>The data support the scope of voucher-based CM intervention to promote engagement with treatment services, and its potential to address the gaps in the care continuum in ARLD. The findings are of practical significance for developing person-centered, tailored interventions for this clinical population. The outcomes of this investigation can inform decision-making among stakeholders and healthcare providers and improve health outcomes for this clinical population.</p>\\n </section>\\n </div>\",\"PeriodicalId\":72145,\"journal\":{\"name\":\"Alcohol (Hanover, York County, Pa.)\",\"volume\":\"48 11\",\"pages\":\"2160-2174\"},\"PeriodicalIF\":2.7000,\"publicationDate\":\"2024-09-26\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/acer.15450\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Alcohol (Hanover, York County, Pa.)\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/acer.15450\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"SUBSTANCE ABUSE\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Alcohol (Hanover, York County, Pa.)","FirstCategoryId":"1085","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/acer.15450","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"SUBSTANCE ABUSE","Score":null,"Total":0}
Voucher-based contingency management to promote treatment engagement in comorbid alcohol use disorder and alcohol-related liver disease: A pilot theory-informed qualitative study with service users
Background
Effective interventions for the management of alcohol-related liver disease (ARLD) remain a gap in clinical practice, and patients' engagement with alcohol services is suboptimal. Based upon the principles of operant conditioning, contingency management (CM) is a psychosocial intervention th at involves gradual, increasing incentives upon completion of treatment-related goals such as treatment attendance.
Methods
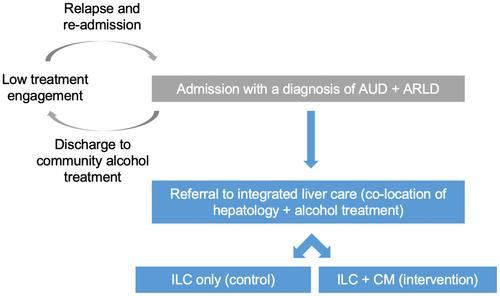
A pilot feasibility trial was conducted with 30 adult patients recruited from an inpatient clinical setting. Consecutive sampling was used to recruit patients presenting comorbid alcohol use disorder (AUD) and ARLD. Participants were randomized to integrated liver care (ILC), receiving hepatology and AUD care, or ILC with a voucher-based CM intervention (intervention arm). A longitudinal qualitative approach was adopted to explore anticipated (Stage 1) and experienced acceptability (Stage 2). The Theoretical Framework of Acceptability (TFA) guided semi-structured in-depth interviews and deductive analysis.
Results
Thirty participants were enrolled in the pilot trial, and interviews were conducted with 24 participants at Stage 1 and seven at Stage 2. Over half of the cohort (54.2%, n = 13) presented decompensated liver disease, and an average of 179 units of alcohol were consumed per week. Overall positive views toward voucher-based CM were noted, and explanatory data emerged across five TFA domains (intervention coherence, ethicality, self-efficacy, perceived effectiveness, and affective attitude). The core aspects of the voucher-based CM intervention matched participants' preferences and needs. Participants regarded CM as having a symbolic value and strengthening the therapeutic alliance with healthcare providers.
Conclusion
The data support the scope of voucher-based CM intervention to promote engagement with treatment services, and its potential to address the gaps in the care continuum in ARLD. The findings are of practical significance for developing person-centered, tailored interventions for this clinical population. The outcomes of this investigation can inform decision-making among stakeholders and healthcare providers and improve health outcomes for this clinical population.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


