{"title":"揭示全髋关节置换术术中污染的动态变化:微粒污染与微生物污染在手术部位感染风险中的差异。","authors":"Toshiyuki Tateiwa, Toshinori Masaoka, Yasuhito Takahashi, Tsunehito Ishida, Takaaki Shishido, Kengo Yamamoto","doi":"10.1186/s42836-024-00272-0","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Surgical site infection (SSI) is a major problem following total hip arthroplasty (THA). This study investigated the impact of a standard intraoperative routine where the surgical team wears full-body exhaust suits (space suits) within a laminar airflow (LAF)-ventilated operating room (OR) on environmental contamination. Our primary objective was to identify potential modifiable intraoperative factors that could be better controlled to minimize SSI risk.</p><p><strong>Methods: </strong>We implemented an approach involving simultaneous and continuous air sampling throughout actual primary cementless THA procedures. This method concurrently monitored both airborne particle and microbial contamination levels from the time the patient entered the OR for surgery until extubation.</p><p><strong>Results: </strong>Airborne particulate and microbial contamination significantly increased during the first and second patient repositionings (postural changes) when the surgical team was not wearing space suits. However, their concentration exhibited inconsistent changes during the core surgical procedures, between incision and suturing, when the surgeons wore space suits. The microbial biosensor detected zero median microbes from draping to suturing. In contrast, the particle counter indicated a significant level of airborne particles during head resection and cup press-fitting, suggesting these procedures might generate more non-viable particles.</p><p><strong>Conclusions: </strong>This study identified a significant portion of airborne particles during the core surgical procedures as non-viable, suggesting that monitoring solely for particle counts might not suffice to estimate SSI risk. Our findings strongly support the use of space suits for surgeons to minimize intraoperative microbial contamination within LAF-ventilated ORs. Therefore, minimizing unnecessary traffic and movement of unsterile personnel is crucial. Additionally, since our data suggest increased contamination during patient repositioning, effectively controlling contamination during the first postural change plays a key role in maintaining low microbial contamination levels throughout the surgery. The use of sterile gowns during this initial maneuver might further reduce SSIs. Further research is warranted to investigate the impact of sterile attire on SSIs.</p>","PeriodicalId":52831,"journal":{"name":"Arthroplasty","volume":"6 1","pages":"49"},"PeriodicalIF":4.3000,"publicationDate":"2024-10-01","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11443724/pdf/","citationCount":"0","resultStr":"{\"title\":\"Unveiling the dynamics of intraoperative contamination in total hip arthroplasty: the discrepancy between particulate and microbial contamination in surgical site infection risk.\",\"authors\":\"Toshiyuki Tateiwa, Toshinori Masaoka, Yasuhito Takahashi, Tsunehito Ishida, Takaaki Shishido, Kengo Yamamoto\",\"doi\":\"10.1186/s42836-024-00272-0\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Surgical site infection (SSI) is a major problem following total hip arthroplasty (THA). This study investigated the impact of a standard intraoperative routine where the surgical team wears full-body exhaust suits (space suits) within a laminar airflow (LAF)-ventilated operating room (OR) on environmental contamination. Our primary objective was to identify potential modifiable intraoperative factors that could be better controlled to minimize SSI risk.</p><p><strong>Methods: </strong>We implemented an approach involving simultaneous and continuous air sampling throughout actual primary cementless THA procedures. This method concurrently monitored both airborne particle and microbial contamination levels from the time the patient entered the OR for surgery until extubation.</p><p><strong>Results: </strong>Airborne particulate and microbial contamination significantly increased during the first and second patient repositionings (postural changes) when the surgical team was not wearing space suits. However, their concentration exhibited inconsistent changes during the core surgical procedures, between incision and suturing, when the surgeons wore space suits. The microbial biosensor detected zero median microbes from draping to suturing. In contrast, the particle counter indicated a significant level of airborne particles during head resection and cup press-fitting, suggesting these procedures might generate more non-viable particles.</p><p><strong>Conclusions: </strong>This study identified a significant portion of airborne particles during the core surgical procedures as non-viable, suggesting that monitoring solely for particle counts might not suffice to estimate SSI risk. Our findings strongly support the use of space suits for surgeons to minimize intraoperative microbial contamination within LAF-ventilated ORs. Therefore, minimizing unnecessary traffic and movement of unsterile personnel is crucial. Additionally, since our data suggest increased contamination during patient repositioning, effectively controlling contamination during the first postural change plays a key role in maintaining low microbial contamination levels throughout the surgery. The use of sterile gowns during this initial maneuver might further reduce SSIs. Further research is warranted to investigate the impact of sterile attire on SSIs.</p>\",\"PeriodicalId\":52831,\"journal\":{\"name\":\"Arthroplasty\",\"volume\":\"6 1\",\"pages\":\"49\"},\"PeriodicalIF\":4.3000,\"publicationDate\":\"2024-10-01\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11443724/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Arthroplasty\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s42836-024-00272-0\",\"RegionNum\":4,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"ORTHOPEDICS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Arthroplasty","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s42836-024-00272-0","RegionNum":4,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"ORTHOPEDICS","Score":null,"Total":0}
Unveiling the dynamics of intraoperative contamination in total hip arthroplasty: the discrepancy between particulate and microbial contamination in surgical site infection risk.
Background: Surgical site infection (SSI) is a major problem following total hip arthroplasty (THA). This study investigated the impact of a standard intraoperative routine where the surgical team wears full-body exhaust suits (space suits) within a laminar airflow (LAF)-ventilated operating room (OR) on environmental contamination. Our primary objective was to identify potential modifiable intraoperative factors that could be better controlled to minimize SSI risk.
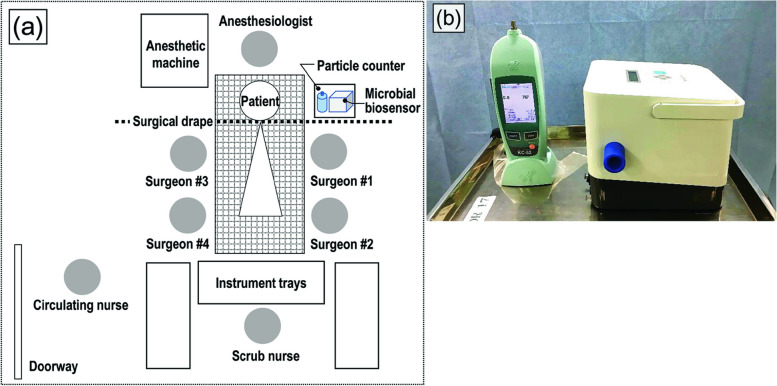
Methods: We implemented an approach involving simultaneous and continuous air sampling throughout actual primary cementless THA procedures. This method concurrently monitored both airborne particle and microbial contamination levels from the time the patient entered the OR for surgery until extubation.
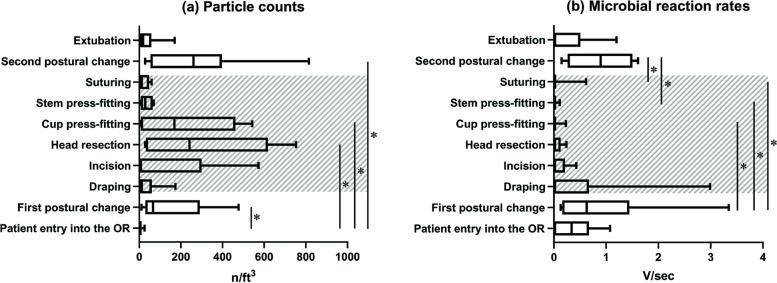
Results: Airborne particulate and microbial contamination significantly increased during the first and second patient repositionings (postural changes) when the surgical team was not wearing space suits. However, their concentration exhibited inconsistent changes during the core surgical procedures, between incision and suturing, when the surgeons wore space suits. The microbial biosensor detected zero median microbes from draping to suturing. In contrast, the particle counter indicated a significant level of airborne particles during head resection and cup press-fitting, suggesting these procedures might generate more non-viable particles.
Conclusions: This study identified a significant portion of airborne particles during the core surgical procedures as non-viable, suggesting that monitoring solely for particle counts might not suffice to estimate SSI risk. Our findings strongly support the use of space suits for surgeons to minimize intraoperative microbial contamination within LAF-ventilated ORs. Therefore, minimizing unnecessary traffic and movement of unsterile personnel is crucial. Additionally, since our data suggest increased contamination during patient repositioning, effectively controlling contamination during the first postural change plays a key role in maintaining low microbial contamination levels throughout the surgery. The use of sterile gowns during this initial maneuver might further reduce SSIs. Further research is warranted to investigate the impact of sterile attire on SSIs.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


