Jared A Daar, Yoshiya Toyoda, Norihisa Shigemura, Sean M Baskin, Parag Desai, Matthew Gordon
{"title":"体外膜肺氧合作为肺移植的桥梁:大型老年队列中的 5 年疗效和决定桥梁。","authors":"Jared A Daar, Yoshiya Toyoda, Norihisa Shigemura, Sean M Baskin, Parag Desai, Matthew Gordon","doi":"10.1186/s12931-024-02968-y","DOIUrl":null,"url":null,"abstract":"<p><strong>Background: </strong>Extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplantation (BTT) has expanded considerably, though evidence-based selection criteria and long-term outcome data are lacking. The purpose of this study was to evaluate whether risk factors often used to exclude patients from ECMO BTT-specifically older age and not yet being listed for transplant-are validated by long-term outcomes.</p><p><strong>Methods: </strong>To ensure minimum 5-year follow-up, a retrospective cohort study was performed of adult patients actively listed for lung transplantation at a high-volume center and bridged on ECMO between January 2012 and December 2017. Data was collected through January 1, 2023.</p><p><strong>Results: </strong>Among 50 patients bridged on ECMO, 25 survived to transplant. Median age at listing was 58 (interquartile range [IQR], 42-65) in the transplanted group and 65 (IQR, 56.5-69) in the deceased group (P = 0.051). One-year, 3-year, and 5-year survival were 88% (22/25), 60% (15/25), and 44% (11/25), respectively, with eight patients still living at the time of review. Median time spent at home during the year post-transplant was 340 days (IQR, 314-355). Older age at listing was a negative predictor of survival on ECMO to transplant (odds ratio 0.92 [95% confidence interval, 0.86-0.99], P = 0.01). Thirteen patients were placed on ECMO prior to being listed and three were listed the same day as ECMO cannulation, with 10/16 transplanted. No significant difference in post-transplant survival was found between patients placed on ECMO prior to listing (n = 10) and those already listed (n = 15) (P = 0.93, log-rank). Serial post-transplant spirometry up to 5 years and surveillance transbronchial biopsy demonstrated good allograft function and low rates of cellular rejection.</p><p><strong>Conclusions: </strong>In one of the oldest cohorts of ECMO BTT patients described, favorable survival outcomes and allograft function were observed up to 5 years irrespective of whether patients were previously listed or bridged to decision. Despite inherent limitations to this retrospective, single-center study, the data presented support the feasibility of ECMO BTT in older and not previously listed advanced lung disease patients.</p>","PeriodicalId":49131,"journal":{"name":"Respiratory Research","volume":"25 1","pages":"350"},"PeriodicalIF":5.8000,"publicationDate":"2024-09-28","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11439265/pdf/","citationCount":"0","resultStr":"{\"title\":\"Extracorporeal membrane oxygenation as a bridge to lung transplantation: 5-year outcomes and bridge to decision in a large, older cohort.\",\"authors\":\"Jared A Daar, Yoshiya Toyoda, Norihisa Shigemura, Sean M Baskin, Parag Desai, Matthew Gordon\",\"doi\":\"10.1186/s12931-024-02968-y\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Background: </strong>Extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplantation (BTT) has expanded considerably, though evidence-based selection criteria and long-term outcome data are lacking. The purpose of this study was to evaluate whether risk factors often used to exclude patients from ECMO BTT-specifically older age and not yet being listed for transplant-are validated by long-term outcomes.</p><p><strong>Methods: </strong>To ensure minimum 5-year follow-up, a retrospective cohort study was performed of adult patients actively listed for lung transplantation at a high-volume center and bridged on ECMO between January 2012 and December 2017. Data was collected through January 1, 2023.</p><p><strong>Results: </strong>Among 50 patients bridged on ECMO, 25 survived to transplant. Median age at listing was 58 (interquartile range [IQR], 42-65) in the transplanted group and 65 (IQR, 56.5-69) in the deceased group (P = 0.051). One-year, 3-year, and 5-year survival were 88% (22/25), 60% (15/25), and 44% (11/25), respectively, with eight patients still living at the time of review. Median time spent at home during the year post-transplant was 340 days (IQR, 314-355). Older age at listing was a negative predictor of survival on ECMO to transplant (odds ratio 0.92 [95% confidence interval, 0.86-0.99], P = 0.01). Thirteen patients were placed on ECMO prior to being listed and three were listed the same day as ECMO cannulation, with 10/16 transplanted. No significant difference in post-transplant survival was found between patients placed on ECMO prior to listing (n = 10) and those already listed (n = 15) (P = 0.93, log-rank). Serial post-transplant spirometry up to 5 years and surveillance transbronchial biopsy demonstrated good allograft function and low rates of cellular rejection.</p><p><strong>Conclusions: </strong>In one of the oldest cohorts of ECMO BTT patients described, favorable survival outcomes and allograft function were observed up to 5 years irrespective of whether patients were previously listed or bridged to decision. Despite inherent limitations to this retrospective, single-center study, the data presented support the feasibility of ECMO BTT in older and not previously listed advanced lung disease patients.</p>\",\"PeriodicalId\":49131,\"journal\":{\"name\":\"Respiratory Research\",\"volume\":\"25 1\",\"pages\":\"350\"},\"PeriodicalIF\":5.8000,\"publicationDate\":\"2024-09-28\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11439265/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Respiratory Research\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1186/s12931-024-02968-y\",\"RegionNum\":2,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Respiratory Research","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1186/s12931-024-02968-y","RegionNum":2,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"Medicine","Score":null,"Total":0}
Extracorporeal membrane oxygenation as a bridge to lung transplantation: 5-year outcomes and bridge to decision in a large, older cohort.
Background: Extracorporeal membrane oxygenation (ECMO) as a bridge to lung transplantation (BTT) has expanded considerably, though evidence-based selection criteria and long-term outcome data are lacking. The purpose of this study was to evaluate whether risk factors often used to exclude patients from ECMO BTT-specifically older age and not yet being listed for transplant-are validated by long-term outcomes.
Methods: To ensure minimum 5-year follow-up, a retrospective cohort study was performed of adult patients actively listed for lung transplantation at a high-volume center and bridged on ECMO between January 2012 and December 2017. Data was collected through January 1, 2023.
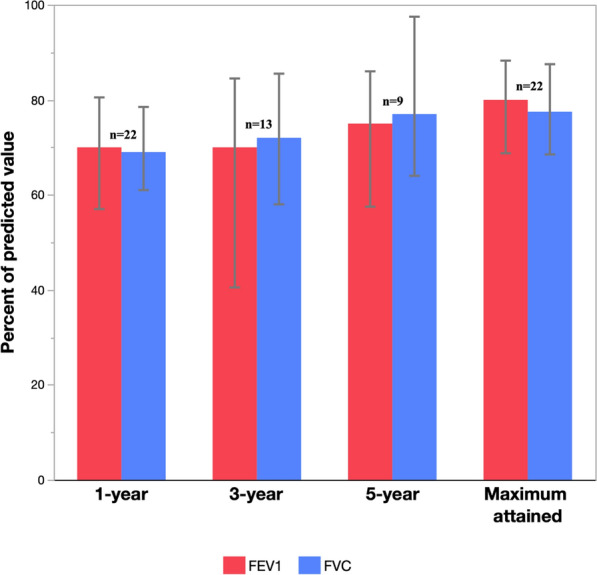
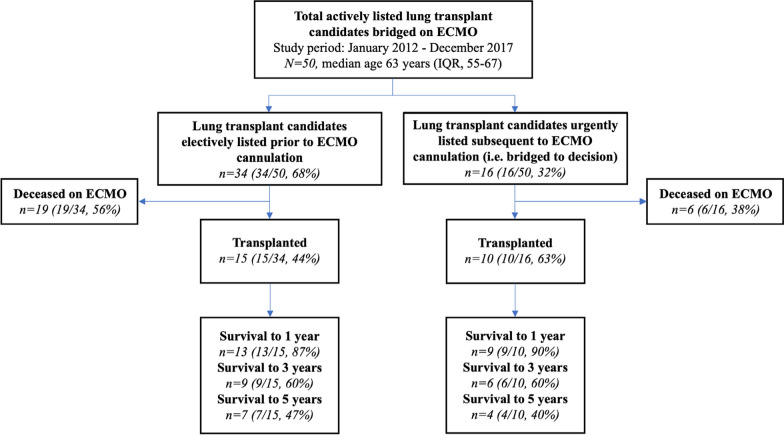
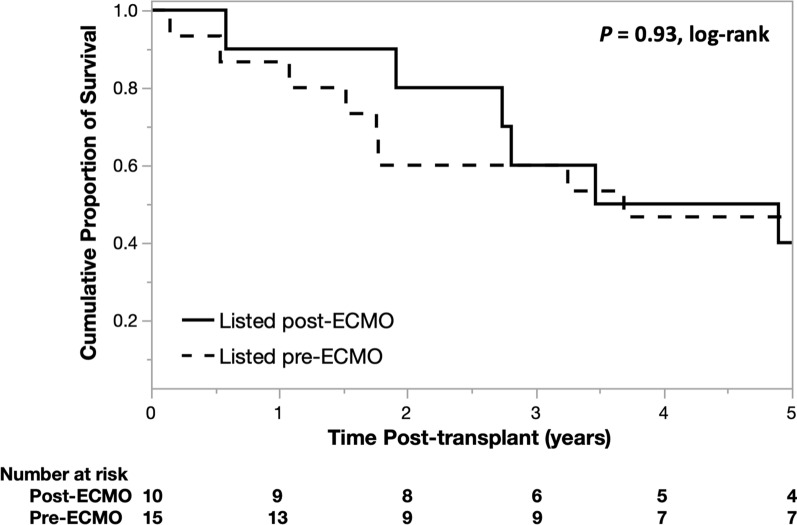
Results: Among 50 patients bridged on ECMO, 25 survived to transplant. Median age at listing was 58 (interquartile range [IQR], 42-65) in the transplanted group and 65 (IQR, 56.5-69) in the deceased group (P = 0.051). One-year, 3-year, and 5-year survival were 88% (22/25), 60% (15/25), and 44% (11/25), respectively, with eight patients still living at the time of review. Median time spent at home during the year post-transplant was 340 days (IQR, 314-355). Older age at listing was a negative predictor of survival on ECMO to transplant (odds ratio 0.92 [95% confidence interval, 0.86-0.99], P = 0.01). Thirteen patients were placed on ECMO prior to being listed and three were listed the same day as ECMO cannulation, with 10/16 transplanted. No significant difference in post-transplant survival was found between patients placed on ECMO prior to listing (n = 10) and those already listed (n = 15) (P = 0.93, log-rank). Serial post-transplant spirometry up to 5 years and surveillance transbronchial biopsy demonstrated good allograft function and low rates of cellular rejection.
Conclusions: In one of the oldest cohorts of ECMO BTT patients described, favorable survival outcomes and allograft function were observed up to 5 years irrespective of whether patients were previously listed or bridged to decision. Despite inherent limitations to this retrospective, single-center study, the data presented support the feasibility of ECMO BTT in older and not previously listed advanced lung disease patients.
期刊介绍:
Respiratory Research publishes high-quality clinical and basic research, review and commentary articles on all aspects of respiratory medicine and related diseases.
As the leading fully open access journal in the field, Respiratory Research provides an essential resource for pulmonologists, allergists, immunologists and other physicians, researchers, healthcare workers and medical students with worldwide dissemination of articles resulting in high visibility and generating international discussion.
Topics of specific interest include asthma, chronic obstructive pulmonary disease, cystic fibrosis, genetics, infectious diseases, interstitial lung diseases, lung development, lung tumors, occupational and environmental factors, pulmonary circulation, pulmonary pharmacology and therapeutics, respiratory immunology, respiratory physiology, and sleep-related respiratory problems.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


