F. D. Richard Hobbs, Richard J. McManus, Clare J. Taylor, Nicholas R. Jones, Joy K. Rahman, Jane Wolstenholme, Sungwook Kim, Joseph Kwon, Louise Jones, Jennifer A. Hirst, Ly-Mee Yu, Sam Mort
{"title":"小剂量螺内酯与中度慢性肾病患者的心血管预后:随机对照试验","authors":"F. D. Richard Hobbs, Richard J. McManus, Clare J. Taylor, Nicholas R. Jones, Joy K. Rahman, Jane Wolstenholme, Sungwook Kim, Joseph Kwon, Louise Jones, Jennifer A. Hirst, Ly-Mee Yu, Sam Mort","doi":"10.1038/s41591-024-03263-5","DOIUrl":null,"url":null,"abstract":"<p>Chronic kidney disease (CKD) is associated with a substantial risk of progression to end-stage renal disease and vascular events. The nonsteroidal mineralocorticoid receptor antagonist (MRA), finerenone, offers cardiorenal protection for people with CKD and diabetes, but there is uncertainty if the steroidal MRA, spironolactone, provides the same protection. In this prospective, randomized, open, blinded endpoint trial, we assessed the effectiveness of 25 mg spironolactone in addition to usual care or usual care alone for reducing cardiovascular outcomes in stage 3b CKD among an older community cohort (mean age = 74.8 years and s.d. = 8.1). We recruited 1,434 adults from English primary care, of whom 1,372 (96%) were included in the primary analysis. The primary outcome was time from randomization until the first occurrence of death, hospitalization for heart disease, stroke, heart failure, transient ischemic attack or peripheral arterial disease, or first onset of any condition listed not present at baseline. Across 3 years of follow-up, the primary endpoint occurred in 113 of 677 participants randomized to spironolactone (16.7%) and 111 of 695 participants randomized to usual care (16.0%) with no significant difference between groups (hazard ratio = 1.05, 95% confidence interval: 0.81–1.37). Two-thirds of participants randomized to spironolactone stopped treatment within 6 months, predominantly because they met prespecified safety stop criteria. The most common reason for stopping spironolactone was a decrease in the estimated glomerular filtration rate that met prespecified stop criteria (<i>n</i> = 239, 35.4%), followed by participants being withdrawn due to treatment side effects (<i>n</i> = 128, 18.9%) and hyperkalemia (<i>n</i> = 54, 8.0%). In conclusion, we found that spironolactone was frequently discontinued due to safety concerns, with no evidence that it reduced cardiovascular outcomes in people with stage 3b CKD. Spironolactone should not be used for people with stage 3b CKD without another explicit treatment indication. ClinicalTrials.gov registration: ISRCTN44522369.</p>","PeriodicalId":19037,"journal":{"name":"Nature Medicine","volume":null,"pages":null},"PeriodicalIF":58.7000,"publicationDate":"2024-09-30","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Low-dose spironolactone and cardiovascular outcomes in moderate stage chronic kidney disease: a randomized controlled trial\",\"authors\":\"F. D. Richard Hobbs, Richard J. McManus, Clare J. Taylor, Nicholas R. Jones, Joy K. Rahman, Jane Wolstenholme, Sungwook Kim, Joseph Kwon, Louise Jones, Jennifer A. Hirst, Ly-Mee Yu, Sam Mort\",\"doi\":\"10.1038/s41591-024-03263-5\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Chronic kidney disease (CKD) is associated with a substantial risk of progression to end-stage renal disease and vascular events. The nonsteroidal mineralocorticoid receptor antagonist (MRA), finerenone, offers cardiorenal protection for people with CKD and diabetes, but there is uncertainty if the steroidal MRA, spironolactone, provides the same protection. In this prospective, randomized, open, blinded endpoint trial, we assessed the effectiveness of 25 mg spironolactone in addition to usual care or usual care alone for reducing cardiovascular outcomes in stage 3b CKD among an older community cohort (mean age = 74.8 years and s.d. = 8.1). We recruited 1,434 adults from English primary care, of whom 1,372 (96%) were included in the primary analysis. The primary outcome was time from randomization until the first occurrence of death, hospitalization for heart disease, stroke, heart failure, transient ischemic attack or peripheral arterial disease, or first onset of any condition listed not present at baseline. Across 3 years of follow-up, the primary endpoint occurred in 113 of 677 participants randomized to spironolactone (16.7%) and 111 of 695 participants randomized to usual care (16.0%) with no significant difference between groups (hazard ratio = 1.05, 95% confidence interval: 0.81–1.37). Two-thirds of participants randomized to spironolactone stopped treatment within 6 months, predominantly because they met prespecified safety stop criteria. The most common reason for stopping spironolactone was a decrease in the estimated glomerular filtration rate that met prespecified stop criteria (<i>n</i> = 239, 35.4%), followed by participants being withdrawn due to treatment side effects (<i>n</i> = 128, 18.9%) and hyperkalemia (<i>n</i> = 54, 8.0%). In conclusion, we found that spironolactone was frequently discontinued due to safety concerns, with no evidence that it reduced cardiovascular outcomes in people with stage 3b CKD. Spironolactone should not be used for people with stage 3b CKD without another explicit treatment indication. ClinicalTrials.gov registration: ISRCTN44522369.</p>\",\"PeriodicalId\":19037,\"journal\":{\"name\":\"Nature Medicine\",\"volume\":null,\"pages\":null},\"PeriodicalIF\":58.7000,\"publicationDate\":\"2024-09-30\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Nature Medicine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1038/s41591-024-03263-5\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"BIOCHEMISTRY & MOLECULAR BIOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Nature Medicine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1038/s41591-024-03263-5","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"BIOCHEMISTRY & MOLECULAR BIOLOGY","Score":null,"Total":0}
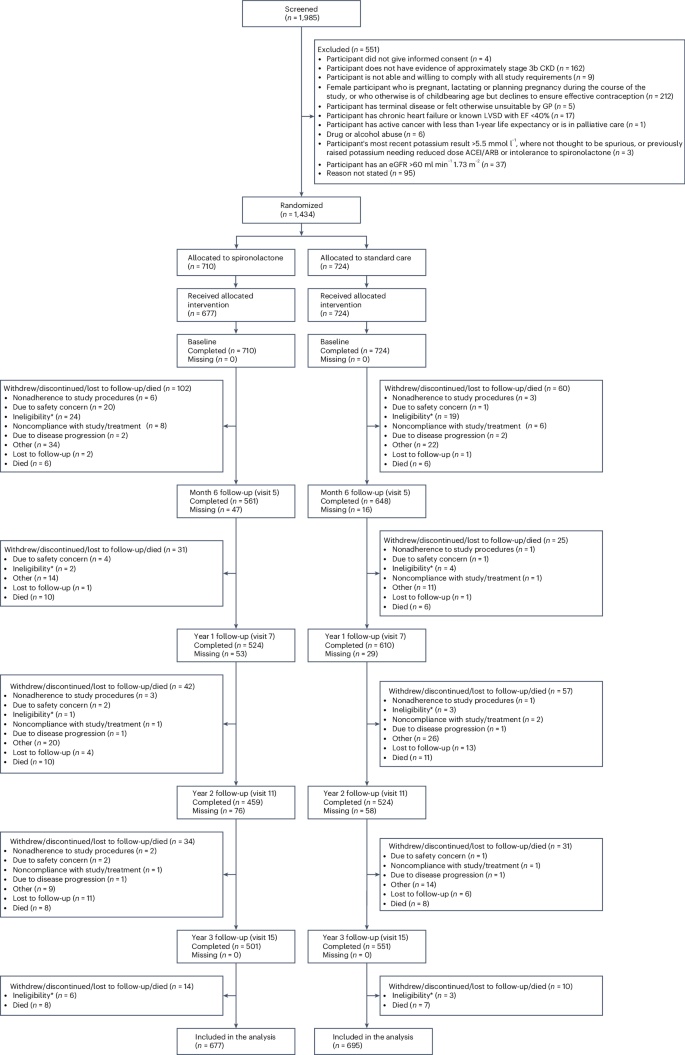
Low-dose spironolactone and cardiovascular outcomes in moderate stage chronic kidney disease: a randomized controlled trial
Chronic kidney disease (CKD) is associated with a substantial risk of progression to end-stage renal disease and vascular events. The nonsteroidal mineralocorticoid receptor antagonist (MRA), finerenone, offers cardiorenal protection for people with CKD and diabetes, but there is uncertainty if the steroidal MRA, spironolactone, provides the same protection. In this prospective, randomized, open, blinded endpoint trial, we assessed the effectiveness of 25 mg spironolactone in addition to usual care or usual care alone for reducing cardiovascular outcomes in stage 3b CKD among an older community cohort (mean age = 74.8 years and s.d. = 8.1). We recruited 1,434 adults from English primary care, of whom 1,372 (96%) were included in the primary analysis. The primary outcome was time from randomization until the first occurrence of death, hospitalization for heart disease, stroke, heart failure, transient ischemic attack or peripheral arterial disease, or first onset of any condition listed not present at baseline. Across 3 years of follow-up, the primary endpoint occurred in 113 of 677 participants randomized to spironolactone (16.7%) and 111 of 695 participants randomized to usual care (16.0%) with no significant difference between groups (hazard ratio = 1.05, 95% confidence interval: 0.81–1.37). Two-thirds of participants randomized to spironolactone stopped treatment within 6 months, predominantly because they met prespecified safety stop criteria. The most common reason for stopping spironolactone was a decrease in the estimated glomerular filtration rate that met prespecified stop criteria (n = 239, 35.4%), followed by participants being withdrawn due to treatment side effects (n = 128, 18.9%) and hyperkalemia (n = 54, 8.0%). In conclusion, we found that spironolactone was frequently discontinued due to safety concerns, with no evidence that it reduced cardiovascular outcomes in people with stage 3b CKD. Spironolactone should not be used for people with stage 3b CKD without another explicit treatment indication. ClinicalTrials.gov registration: ISRCTN44522369.
期刊介绍:
Nature Medicine is a monthly journal publishing original peer-reviewed research in all areas of medicine. The publication focuses on originality, timeliness, interdisciplinary interest, and the impact on improving human health. In addition to research articles, Nature Medicine also publishes commissioned content such as News, Reviews, and Perspectives. This content aims to provide context for the latest advances in translational and clinical research, reaching a wide audience of M.D. and Ph.D. readers. All editorial decisions for the journal are made by a team of full-time professional editors.
Nature Medicine consider all types of clinical research, including:
-Case-reports and small case series
-Clinical trials, whether phase 1, 2, 3 or 4
-Observational studies
-Meta-analyses
-Biomarker studies
-Public and global health studies
Nature Medicine is also committed to facilitating communication between translational and clinical researchers. As such, we consider “hybrid” studies with preclinical and translational findings reported alongside data from clinical studies.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


