Oreoluwa E Olakunle, Rachel S Tobin, Nicole Guynn, Anita Osabutey, Maya Younker, Mahnoor Khan, Marina Mosunjac, Alison F Ward, Modele O Ogunniyi
{"title":"收缩的心脏一名 31 岁男子的缩窄性结核性心包炎病例。","authors":"Oreoluwa E Olakunle, Rachel S Tobin, Nicole Guynn, Anita Osabutey, Maya Younker, Mahnoor Khan, Marina Mosunjac, Alison F Ward, Modele O Ogunniyi","doi":"10.12659/AJCR.944607","DOIUrl":null,"url":null,"abstract":"<p><p>BACKGROUND Constrictive pericarditis occurs due to chronic pericardial inflammation and adherence of the cardiac pericardial layer. Etiologies include toxins, infection, cardiac surgery, and idiopathic causes. Outside the United States, the most common cause of constrictive pericarditis is tuberculosis (TB). Constrictive pericarditis is the most severe complication of tuberculous pericardial disease. CASE REPORT A 31-year-old man who recently immigrated to the United States presented with a 2-week history of constitutional symptoms, dyspnea, and pleuritic chest pain. Physical examination was pertinent for bilateral lower extremity pitting edema, decreased bilateral breath sounds, and jugular venous distension. Transthoracic echocardiogram revealed a left ventricular ejection fraction of 45%, pericardial thickening, and an exaggerated septal bounce. Right heart catheterization showed discordant and concordant right ventricular pressure tracings. Cardiac magnetic resonance imaging revealed bilateral pleural effusions and circumferential pericardial thickening. Thoracocentesis was significant for an exudative effusion, with elevated adenosine deaminase levels. Subsequent QuantiFERON-TB Gold testing was positive, and he underwent elective pericardiectomy. Pericardial histopathology revealed necrotizing caseating granulomas. He was discharged on a 6-month course of rifampicin, isoniazid, pyrazinamide, and ethambutol therapy, with close multidisciplinary care team outpatient follow-up. CONCLUSIONS This case highlights the importance of a high index of clinical suspicion for tuberculous pericarditis in patients presenting with constitutional and heart failure symptoms and a relevant travel history, to ensure prompt diagnosis and treatment. This case also reflects the importance of coordination of care between cardiology, infectious disease, pathology, and cardiothoracic surgery teams in the management of tuberculous constrictive pericarditis.</p>","PeriodicalId":39064,"journal":{"name":"American Journal of Case Reports","volume":"25 ","pages":"e944607"},"PeriodicalIF":0.7000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11437574/pdf/","citationCount":"0","resultStr":"{\"title\":\"The Constricted Heart: A 31-Year-Old Man with a Case of Constrictive Tuberculous Pericarditis.\",\"authors\":\"Oreoluwa E Olakunle, Rachel S Tobin, Nicole Guynn, Anita Osabutey, Maya Younker, Mahnoor Khan, Marina Mosunjac, Alison F Ward, Modele O Ogunniyi\",\"doi\":\"10.12659/AJCR.944607\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><p>BACKGROUND Constrictive pericarditis occurs due to chronic pericardial inflammation and adherence of the cardiac pericardial layer. Etiologies include toxins, infection, cardiac surgery, and idiopathic causes. Outside the United States, the most common cause of constrictive pericarditis is tuberculosis (TB). Constrictive pericarditis is the most severe complication of tuberculous pericardial disease. CASE REPORT A 31-year-old man who recently immigrated to the United States presented with a 2-week history of constitutional symptoms, dyspnea, and pleuritic chest pain. Physical examination was pertinent for bilateral lower extremity pitting edema, decreased bilateral breath sounds, and jugular venous distension. Transthoracic echocardiogram revealed a left ventricular ejection fraction of 45%, pericardial thickening, and an exaggerated septal bounce. Right heart catheterization showed discordant and concordant right ventricular pressure tracings. Cardiac magnetic resonance imaging revealed bilateral pleural effusions and circumferential pericardial thickening. Thoracocentesis was significant for an exudative effusion, with elevated adenosine deaminase levels. Subsequent QuantiFERON-TB Gold testing was positive, and he underwent elective pericardiectomy. Pericardial histopathology revealed necrotizing caseating granulomas. He was discharged on a 6-month course of rifampicin, isoniazid, pyrazinamide, and ethambutol therapy, with close multidisciplinary care team outpatient follow-up. CONCLUSIONS This case highlights the importance of a high index of clinical suspicion for tuberculous pericarditis in patients presenting with constitutional and heart failure symptoms and a relevant travel history, to ensure prompt diagnosis and treatment. This case also reflects the importance of coordination of care between cardiology, infectious disease, pathology, and cardiothoracic surgery teams in the management of tuberculous constrictive pericarditis.</p>\",\"PeriodicalId\":39064,\"journal\":{\"name\":\"American Journal of Case Reports\",\"volume\":\"25 \",\"pages\":\"e944607\"},\"PeriodicalIF\":0.7000,\"publicationDate\":\"2024-09-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://www.ncbi.nlm.nih.gov/pmc/articles/PMC11437574/pdf/\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"American Journal of Case Reports\",\"FirstCategoryId\":\"1085\",\"ListUrlMain\":\"https://doi.org/10.12659/AJCR.944607\",\"RegionNum\":0,\"RegionCategory\":null,\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q3\",\"JCRName\":\"MEDICINE, GENERAL & INTERNAL\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"American Journal of Case Reports","FirstCategoryId":"1085","ListUrlMain":"https://doi.org/10.12659/AJCR.944607","RegionNum":0,"RegionCategory":null,"ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q3","JCRName":"MEDICINE, GENERAL & INTERNAL","Score":null,"Total":0}
The Constricted Heart: A 31-Year-Old Man with a Case of Constrictive Tuberculous Pericarditis.
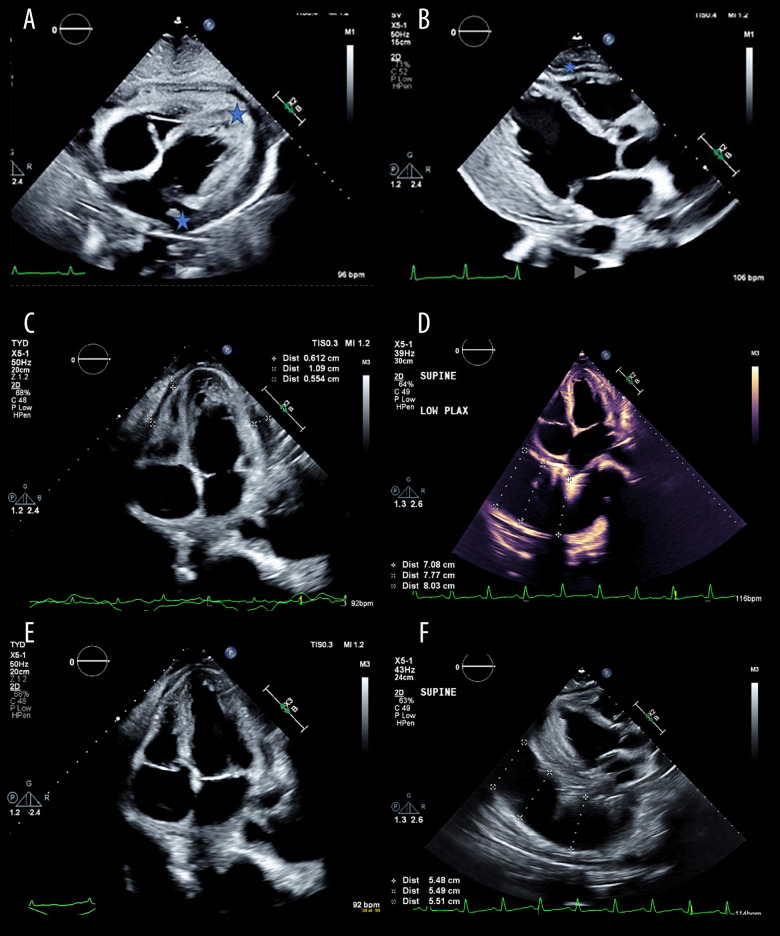
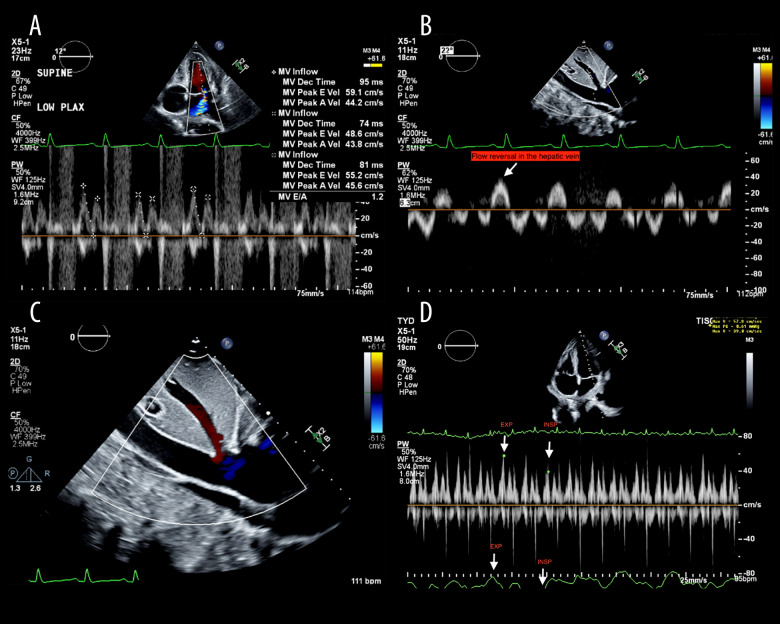
BACKGROUND Constrictive pericarditis occurs due to chronic pericardial inflammation and adherence of the cardiac pericardial layer. Etiologies include toxins, infection, cardiac surgery, and idiopathic causes. Outside the United States, the most common cause of constrictive pericarditis is tuberculosis (TB). Constrictive pericarditis is the most severe complication of tuberculous pericardial disease. CASE REPORT A 31-year-old man who recently immigrated to the United States presented with a 2-week history of constitutional symptoms, dyspnea, and pleuritic chest pain. Physical examination was pertinent for bilateral lower extremity pitting edema, decreased bilateral breath sounds, and jugular venous distension. Transthoracic echocardiogram revealed a left ventricular ejection fraction of 45%, pericardial thickening, and an exaggerated septal bounce. Right heart catheterization showed discordant and concordant right ventricular pressure tracings. Cardiac magnetic resonance imaging revealed bilateral pleural effusions and circumferential pericardial thickening. Thoracocentesis was significant for an exudative effusion, with elevated adenosine deaminase levels. Subsequent QuantiFERON-TB Gold testing was positive, and he underwent elective pericardiectomy. Pericardial histopathology revealed necrotizing caseating granulomas. He was discharged on a 6-month course of rifampicin, isoniazid, pyrazinamide, and ethambutol therapy, with close multidisciplinary care team outpatient follow-up. CONCLUSIONS This case highlights the importance of a high index of clinical suspicion for tuberculous pericarditis in patients presenting with constitutional and heart failure symptoms and a relevant travel history, to ensure prompt diagnosis and treatment. This case also reflects the importance of coordination of care between cardiology, infectious disease, pathology, and cardiothoracic surgery teams in the management of tuberculous constrictive pericarditis.
期刊介绍:
American Journal of Case Reports is an international, peer-reviewed scientific journal that publishes single and series case reports in all medical fields. American Journal of Case Reports is issued on a continuous basis as a primary electronic journal. Print copies of a single article or a set of articles can be ordered on demand.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


