Xiaowen Wang, Maria A Pabon, Maja Cikes, Karola Jering, Wilfried Mullens, Lars Kober, Pardeep S Jhund, Attila Kovacs, Bela Merkely, Yinong Zhou, John J V McMurray, Amil M Shah, Sheila M Hegde, Brian Claggett, Marc A Pfeffer, Scott D Solomon
{"title":"急性心肌梗死后心脏结构和功能的性别差异:PARADISE-MI 超声心动图子研究的启示。","authors":"Xiaowen Wang, Maria A Pabon, Maja Cikes, Karola Jering, Wilfried Mullens, Lars Kober, Pardeep S Jhund, Attila Kovacs, Bela Merkely, Yinong Zhou, John J V McMurray, Amil M Shah, Sheila M Hegde, Brian Claggett, Marc A Pfeffer, Scott D Solomon","doi":"10.1002/ejhf.3472","DOIUrl":null,"url":null,"abstract":"<p><strong>Aims: </strong>The incidence of heart failure hospitalization is higher in women than in men after myocardial infarction (MI). Sex-related differences in left ventricular (LV) remodelling may contribute to the differences in post-MI outcomes. The aim of this study was to assess sex differences in echocardiographic parameters post-MI, and whether the relationship between echocardiographic parameters and clinical outcomes differs by sex.</p><p><strong>Methods and results: </strong>In the PARADISE-MI trial, patients were randomized to sacubitril/valsartan or ramipril within 0.5 to 7 days of high-risk MI. In the pre-specified echocardiographic substudy, 544 patients underwent echocardiography at the time of randomization and after 8 months. We compared key echocardiographic parameters in men and women and their association with primary composite outcome (cardiovascular death or incident heart failure). At baseline, women had higher LV ejection fraction (LVEF), lower LV end-diastolic volume (LVEDV) index, LV end-systolic volume (LVESV) index, and LV mass index. After adjusting for baseline clinical differences, changes in these echocardiographic parameters from baseline to 8 months were not significantly different in women versus men. Lower LVEF, higher LVEDV, LVESV, left atrial volume index, and average E/e' were associated with a higher risk of the primary composite outcome. Sex did not modify the relationship between echocardiographic parameters and clinical outcome.</p><p><strong>Conclusions: </strong>Despite baseline differences in measures of cardiac function between men and women following acute high-risk MI, there were no significant sex-related changes in chamber size or LV function. Sex did not modify the association between echocardiographic parameters and clinical outcome.</p>","PeriodicalId":164,"journal":{"name":"European Journal of Heart Failure","volume":" ","pages":""},"PeriodicalIF":16.9000,"publicationDate":"2024-09-24","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Sex differences in cardiac structure and function following acute myocardial infarction: Insights from the PARADISE-MI echocardiographic substudy.\",\"authors\":\"Xiaowen Wang, Maria A Pabon, Maja Cikes, Karola Jering, Wilfried Mullens, Lars Kober, Pardeep S Jhund, Attila Kovacs, Bela Merkely, Yinong Zhou, John J V McMurray, Amil M Shah, Sheila M Hegde, Brian Claggett, Marc A Pfeffer, Scott D Solomon\",\"doi\":\"10.1002/ejhf.3472\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p><strong>Aims: </strong>The incidence of heart failure hospitalization is higher in women than in men after myocardial infarction (MI). Sex-related differences in left ventricular (LV) remodelling may contribute to the differences in post-MI outcomes. The aim of this study was to assess sex differences in echocardiographic parameters post-MI, and whether the relationship between echocardiographic parameters and clinical outcomes differs by sex.</p><p><strong>Methods and results: </strong>In the PARADISE-MI trial, patients were randomized to sacubitril/valsartan or ramipril within 0.5 to 7 days of high-risk MI. In the pre-specified echocardiographic substudy, 544 patients underwent echocardiography at the time of randomization and after 8 months. We compared key echocardiographic parameters in men and women and their association with primary composite outcome (cardiovascular death or incident heart failure). At baseline, women had higher LV ejection fraction (LVEF), lower LV end-diastolic volume (LVEDV) index, LV end-systolic volume (LVESV) index, and LV mass index. After adjusting for baseline clinical differences, changes in these echocardiographic parameters from baseline to 8 months were not significantly different in women versus men. Lower LVEF, higher LVEDV, LVESV, left atrial volume index, and average E/e' were associated with a higher risk of the primary composite outcome. Sex did not modify the relationship between echocardiographic parameters and clinical outcome.</p><p><strong>Conclusions: </strong>Despite baseline differences in measures of cardiac function between men and women following acute high-risk MI, there were no significant sex-related changes in chamber size or LV function. Sex did not modify the association between echocardiographic parameters and clinical outcome.</p>\",\"PeriodicalId\":164,\"journal\":{\"name\":\"European Journal of Heart Failure\",\"volume\":\" \",\"pages\":\"\"},\"PeriodicalIF\":16.9000,\"publicationDate\":\"2024-09-24\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"European Journal of Heart Failure\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1002/ejhf.3472\",\"RegionNum\":1,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q1\",\"JCRName\":\"CARDIAC & CARDIOVASCULAR SYSTEMS\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"European Journal of Heart Failure","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1002/ejhf.3472","RegionNum":1,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q1","JCRName":"CARDIAC & CARDIOVASCULAR SYSTEMS","Score":null,"Total":0}
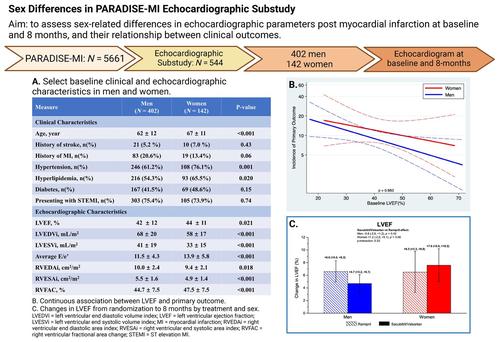
Sex differences in cardiac structure and function following acute myocardial infarction: Insights from the PARADISE-MI echocardiographic substudy.
Aims: The incidence of heart failure hospitalization is higher in women than in men after myocardial infarction (MI). Sex-related differences in left ventricular (LV) remodelling may contribute to the differences in post-MI outcomes. The aim of this study was to assess sex differences in echocardiographic parameters post-MI, and whether the relationship between echocardiographic parameters and clinical outcomes differs by sex.
Methods and results: In the PARADISE-MI trial, patients were randomized to sacubitril/valsartan or ramipril within 0.5 to 7 days of high-risk MI. In the pre-specified echocardiographic substudy, 544 patients underwent echocardiography at the time of randomization and after 8 months. We compared key echocardiographic parameters in men and women and their association with primary composite outcome (cardiovascular death or incident heart failure). At baseline, women had higher LV ejection fraction (LVEF), lower LV end-diastolic volume (LVEDV) index, LV end-systolic volume (LVESV) index, and LV mass index. After adjusting for baseline clinical differences, changes in these echocardiographic parameters from baseline to 8 months were not significantly different in women versus men. Lower LVEF, higher LVEDV, LVESV, left atrial volume index, and average E/e' were associated with a higher risk of the primary composite outcome. Sex did not modify the relationship between echocardiographic parameters and clinical outcome.
Conclusions: Despite baseline differences in measures of cardiac function between men and women following acute high-risk MI, there were no significant sex-related changes in chamber size or LV function. Sex did not modify the association between echocardiographic parameters and clinical outcome.
期刊介绍:
European Journal of Heart Failure is an international journal dedicated to advancing knowledge in the field of heart failure management. The journal publishes reviews and editorials aimed at improving understanding, prevention, investigation, and treatment of heart failure. It covers various disciplines such as molecular and cellular biology, pathology, physiology, electrophysiology, pharmacology, clinical sciences, social sciences, and population sciences. The journal welcomes submissions of manuscripts on basic, clinical, and population sciences, as well as original contributions on nursing, care of the elderly, primary care, health economics, and other related specialist fields. It is published monthly and has a readership that includes cardiologists, emergency room physicians, intensivists, internists, general physicians, cardiac nurses, diabetologists, epidemiologists, basic scientists focusing on cardiovascular research, and those working in rehabilitation. The journal is abstracted and indexed in various databases such as Academic Search, Embase, MEDLINE/PubMed, and Science Citation Index.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


