肝硬化患者非选择性β-受体阻滞剂候选者筛选算法探索:PREDESCI 试验的事后分析。
IF 26.8
1区 医学
Q1 GASTROENTEROLOGY & HEPATOLOGY
引用次数: 0
摘要
背景与目的:非侵入性检查(NIT)能否准确选择需要使用非选择性β-受体阻滞剂(NSBB)治疗临床意义门静脉高压症(CSPH)和预防失代偿的肝硬化患者尚不清楚。我们的目的是利用前瞻性 PREDESCI 队列测试基于 NIT 的 CSPH 诊断算法的性能。我们研究了一种结合 NIT 和内镜检查的新算法,以提高其性能:方法:我们纳入了在试验期间接受筛查的代偿期肝硬化和肝脏弹性成像检查的患者。评估了基于肝脏硬度测量(LSM)和血小板计数的模型的性能。然后开发了一种算法,考虑对结果不确定("灰色区域")的患者进行内镜检查,并在195名脾脏硬度也可用的独立患者队列中进行了验证:我们纳入了来自 PREDESCI 队列的 170 名患者。仅 LSM≥25 kPa(Baveno VII 标准)或 LSM>20 kPa 加血小板减少症(AASLD 标准)即可判定为 CSPH,阳性预测值分别为 88% 和 89%。然而,37%-47%的患者处于灰色区域,面临失代偿或死亡的高风险。对不确定的病例进行内窥镜检查后,发现有静脉曲张的患者被重新归类为 CSPH 的高危人群,从而将灰色区域的比例大幅降至 22%。在这种算法中,86% 的 CSPH 患者被正确归类为高危人群。该算法的诊断性能在外部验证队列中得到了证实,将巴韦诺 VII 标准与脾脏硬度相结合显示出与使用内窥镜的模型相似的准确性:结论:仅以LSM和血小板计数为基础的算法在确定NSBB治疗候选者方面并不理想。对 NIT 检查结果不确定的患者进行内镜检查可提高诊断性能和风险分层。在对灰色区域进行风险分层时,可用脾脏硬度替代内镜检查:PREDESCI试验表明,非选择性β受体阻滞剂可预防CSPH患者的失代偿。我们是否能在不测量 HVPG 的情况下使用非侵入性测试来评估是否存在 CSPH,从而选择治疗候选者,目前仍不清楚。在试验期间筛查的前瞻性患者队列中,我们发现基于肝脏硬度和血小板计数的算法效果不佳,主要原因是不确定结果的比例较高。对灰色区域患者进行内镜检查可显著增加CSPH患者的数量,并改善长期随访中失代偿或死亡的风险分层。这些发现在一个独立的队列中得到了验证。此外,在外部验证队列中,使用脾脏僵硬度代替内镜检查的模型也显示出类似的诊断性能,这表明完全无创的算法可以实现充分的风险分层,以选择治疗候选者。本文章由计算机程序翻译,如有差异,请以英文原文为准。

Exploring algorithms to select candidates for non-selective beta-blockers in cirrhosis: A post hoc analysis of the PREDESCI trial
Background & Aims
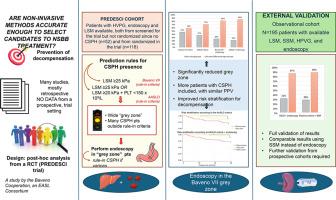
Whether non-invasive tests (NITs) can accurately select patients with cirrhosis requiring non-selective beta-blockers (NSBBs) for clinically significant portal hypertension (CSPH) and prevention of decompensation is unclear. Our aim was to test the performance of NIT-based algorithms for CSPH diagnosis using the prospective PREDESCI cohort. We investigated whether a new algorithm combining NITs with endoscopy could improve performance.
Methods
We included patients with compensated cirrhosis and available liver elastography who were screened during the trial. The performance of models based on liver stiffness measurement (LSM) and platelet count was evaluated. An algorithm considering endoscopy for patients with inconclusive results (the “grey zone”) was then developed and validated in an independent cohort of 195 patients in whom spleen stiffness was also available.
Results
We included 170 patients from the PREDESCI cohort. An LSM ≥25 kPa alone (Baveno VII criteria) or combined with an LSM >20 kPa plus thrombocytopenia (AASLD criteria) ruled-in CSPH with positive predictive values of 88% and 89%, respectively. However, 37%-47% patients fell into the grey zone while at high risk of decompensation or death. Performing endoscopy in inconclusive cases identified patients with varices that, when reclassified as high-risk for CSPH, significantly reduced the grey zone to 22%. In this algorithm, 86% of patients with CSPH were correctly classified as high risk. The diagnostic performance was confirmed in the external validation cohort, where combining Baveno VII criteria with spleen stiffness showed similar accuracy to the model using endoscopy.
Conclusions
Algorithms based only on LSM and platelet count are suboptimal to identify NSBB treatment candidates. Performing endoscopy in patients with indeterminate findings from NITs improved diagnostic performance and risk stratification. Endoscopy may be substituted by spleen stiffness for stratifying risk in the grey zone.
Impact and implications
The PREDESCI trial demonstrated that non-selective beta-blockers prevent decompensation in patients with clinically significant portal hypertension (CSPH). Still, it is unclear whether we can select treatment candidates using non-invasive tests to assess the presence of CSPH without measuring HVPG (hepatic venous pressure gradient). In the prospective cohort of patients screened during the PREDESCI trial, we showed that algorithms based on liver stiffness and platelet count had suboptimal performance, mainly due to a high rate of indeterminate results. Performing endoscopy on patients in the grey zone significantly increased the number correctly characterized as having CSPH and improved the risk stratification for decompensation or death on long-term follow-up. These findings were validated in an independent cohort. In addition, a model using spleen stiffness instead of endoscopy showed similar diagnostic performance in the external validation cohort, suggesting that adequate risk stratification to select treatment candidates can be achieved with a fully non-invasive algorithm.
求助全文
通过发布文献求助,成功后即可免费获取论文全文。
去求助
来源期刊
Journal of Hepatology
医学-胃肠肝病学
CiteScore
46.10
自引率
4.30%
发文量
2325
审稿时长
30 days
期刊介绍:
The Journal of Hepatology is the official publication of the European Association for the Study of the Liver (EASL). It is dedicated to presenting clinical and basic research in the field of hepatology through original papers, reviews, case reports, and letters to the Editor. The Journal is published in English and may consider supplements that pass an editorial review.
 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


