A. Carbone, A. Verrienti, D. S. Cito, C. Corazza, R. Bruno
{"title":"一名甲状腺滤泡癌头颅转移患者 15 年后的 RAI 治疗反应极佳","authors":"A. Carbone, A. Verrienti, D. S. Cito, C. Corazza, R. Bruno","doi":"10.1007/s12020-024-04036-3","DOIUrl":null,"url":null,"abstract":"<p>Bone is the second most common site of metastasis for differentiated thyroid carcinoma (DTC). Bone metastasis (BMs) occur in about 10% of patients with DTC and is observed more often in follicular thyroid carcinoma (FTC) (7–28%) than papillary thyroid carcinoma (PTC) (1–7%). Bone metastasis is associated with unfavorable clinical outcomes mainly including skeletal-related events (SREs), such as pathologic fractures, bone pain, spinal cord compressions, and hypercalcemia, which negatively impact the quality of life of patients and reduce their life expectancy. Patients with BMs from DTC require comprehensive and multimodal treatment approaches, including radioiodine (RAI) therapy, palliative care, surgery, external beam radiotherapy, and targeted drug therapy. RAI therapy is the first-line treatment, despite being rather ineffective, especially in large BMs. The response to RAI therapy, either alone or in combination with BM focal treatment depends on iodine avidity. This study reports a rare case of metachronous skull bone metastasis from FTC in a 72-year-old female patient 15 years after initial treatment. The patient had an excellent response to RAI therapy, which resulted in the abnormal uptake disappearing. Following treatment, the patient has been disease-free for six years. This case confirms that a complete response to RAI treatment for BM depends on the degree of dedifferentiation of cancer cells, which highlights the need for long-term follow-up, especially for FTC patients.</p>","PeriodicalId":11572,"journal":{"name":"Endocrine","volume":"50 1","pages":""},"PeriodicalIF":3.7000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"","citationCount":"0","resultStr":"{\"title\":\"Excellent RAI therapeutic response on a patient presenting skull metastasis of follicular thyroid cancer after 15 years\",\"authors\":\"A. Carbone, A. Verrienti, D. S. Cito, C. Corazza, R. Bruno\",\"doi\":\"10.1007/s12020-024-04036-3\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<p>Bone is the second most common site of metastasis for differentiated thyroid carcinoma (DTC). Bone metastasis (BMs) occur in about 10% of patients with DTC and is observed more often in follicular thyroid carcinoma (FTC) (7–28%) than papillary thyroid carcinoma (PTC) (1–7%). Bone metastasis is associated with unfavorable clinical outcomes mainly including skeletal-related events (SREs), such as pathologic fractures, bone pain, spinal cord compressions, and hypercalcemia, which negatively impact the quality of life of patients and reduce their life expectancy. Patients with BMs from DTC require comprehensive and multimodal treatment approaches, including radioiodine (RAI) therapy, palliative care, surgery, external beam radiotherapy, and targeted drug therapy. RAI therapy is the first-line treatment, despite being rather ineffective, especially in large BMs. The response to RAI therapy, either alone or in combination with BM focal treatment depends on iodine avidity. This study reports a rare case of metachronous skull bone metastasis from FTC in a 72-year-old female patient 15 years after initial treatment. The patient had an excellent response to RAI therapy, which resulted in the abnormal uptake disappearing. Following treatment, the patient has been disease-free for six years. This case confirms that a complete response to RAI treatment for BM depends on the degree of dedifferentiation of cancer cells, which highlights the need for long-term follow-up, especially for FTC patients.</p>\",\"PeriodicalId\":11572,\"journal\":{\"name\":\"Endocrine\",\"volume\":\"50 1\",\"pages\":\"\"},\"PeriodicalIF\":3.7000,\"publicationDate\":\"2024-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Endocrine\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://doi.org/10.1007/s12020-024-04036-3\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"Medicine\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Endocrine","FirstCategoryId":"3","ListUrlMain":"https://doi.org/10.1007/s12020-024-04036-3","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"Medicine","Score":null,"Total":0}
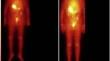
Excellent RAI therapeutic response on a patient presenting skull metastasis of follicular thyroid cancer after 15 years
Bone is the second most common site of metastasis for differentiated thyroid carcinoma (DTC). Bone metastasis (BMs) occur in about 10% of patients with DTC and is observed more often in follicular thyroid carcinoma (FTC) (7–28%) than papillary thyroid carcinoma (PTC) (1–7%). Bone metastasis is associated with unfavorable clinical outcomes mainly including skeletal-related events (SREs), such as pathologic fractures, bone pain, spinal cord compressions, and hypercalcemia, which negatively impact the quality of life of patients and reduce their life expectancy. Patients with BMs from DTC require comprehensive and multimodal treatment approaches, including radioiodine (RAI) therapy, palliative care, surgery, external beam radiotherapy, and targeted drug therapy. RAI therapy is the first-line treatment, despite being rather ineffective, especially in large BMs. The response to RAI therapy, either alone or in combination with BM focal treatment depends on iodine avidity. This study reports a rare case of metachronous skull bone metastasis from FTC in a 72-year-old female patient 15 years after initial treatment. The patient had an excellent response to RAI therapy, which resulted in the abnormal uptake disappearing. Following treatment, the patient has been disease-free for six years. This case confirms that a complete response to RAI treatment for BM depends on the degree of dedifferentiation of cancer cells, which highlights the need for long-term follow-up, especially for FTC patients.
期刊介绍:
Well-established as a major journal in today’s rapidly advancing experimental and clinical research areas, Endocrine publishes original articles devoted to basic (including molecular, cellular and physiological studies), translational and clinical research in all the different fields of endocrinology and metabolism. Articles will be accepted based on peer-reviews, priority, and editorial decision. Invited reviews, mini-reviews and viewpoints on relevant pathophysiological and clinical topics, as well as Editorials on articles appearing in the Journal, are published. Unsolicited Editorials will be evaluated by the editorial team. Outcomes of scientific meetings, as well as guidelines and position statements, may be submitted. The Journal also considers special feature articles in the field of endocrine genetics and epigenetics, as well as articles devoted to novel methods and techniques in endocrinology.
Endocrine covers controversial, clinical endocrine issues. Meta-analyses on endocrine and metabolic topics are also accepted. Descriptions of single clinical cases and/or small patients studies are not published unless of exceptional interest. However, reports of novel imaging studies and endocrine side effects in single patients may be considered. Research letters and letters to the editor related or unrelated to recently published articles can be submitted.
Endocrine covers leading topics in endocrinology such as neuroendocrinology, pituitary and hypothalamic peptides, thyroid physiological and clinical aspects, bone and mineral metabolism and osteoporosis, obesity, lipid and energy metabolism and food intake control, insulin, Type 1 and Type 2 diabetes, hormones of male and female reproduction, adrenal diseases pediatric and geriatric endocrinology, endocrine hypertension and endocrine oncology.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


