Julia F. Kohn, Sonja Boatman, Qi Wang, Schelomo Marmor, Imran Hassan, Robert D. Madoff, Wolfgang B. Gaertner, Paolo Goffredo
{"title":"脾曲腺癌:关于手术切除范围和结果的全国队列分析","authors":"Julia F. Kohn, Sonja Boatman, Qi Wang, Schelomo Marmor, Imran Hassan, Robert D. Madoff, Wolfgang B. Gaertner, Paolo Goffredo","doi":"10.1111/codi.17172","DOIUrl":null,"url":null,"abstract":"<div>\n \n \n <section>\n \n <h3> Aim</h3>\n \n <p>The optimal extent of resection for splenic flexure adenocarcinoma remains debated. These tumours straddle the left- and right-sided vasculature with lymphatic drainage in a watershed area; current guidelines recommend either segmental or extended colectomy. We analysed surgical management of splenic flexure tumours and compared outcomes between approaches.</p>\n </section>\n \n <section>\n \n <h3> Method</h3>\n \n <p>The Surveillance, Epidemiology and End Results database was searched for adults with Stage I–III splenic flexure adenocarcinoma, 2004–2019.</p>\n </section>\n \n <section>\n \n <h3> Results</h3>\n \n <p>Of 5238 patients, 55% underwent extended colectomy. Compared to segmental colectomy, these patients were more likely to have advanced stage. On multivariable analysis, age ≤ 65 years remained independently associated with extended colectomy. Although fewer nodes were examined in segmental colectomy (median 14 vs. 16, <i>p</i> < 0.001), the number of positive nodes (both, median 0 [interquartile ratio 0–2], <i>p</i> = 0.20) and the lymph node ratio were similar between cohorts. Surgical approach was not significantly associated with increased positive nodal yield in adjusted analyses. Five-year overall and disease-specific survival were 73% and 84% for segmental and 72% and 83% for extended colectomy (<i>p</i> > 0.4); these remained comparable after adjustment.</p>\n </section>\n \n <section>\n \n <h3> Conclusions</h3>\n \n <p>Nationally, we observed similar rates of segmental and extended colectomy for splenic flexure adenocarcinoma. Extended colectomy was not more common in Stage III disease, indicating lack of stage migration, and was not associated with better oncological outcomes. These observations support current practice involving either approach, which should be tailored to patient-related factors and preferences, while considering technical aspects and quality of life.</p>\n </section>\n </div>","PeriodicalId":10512,"journal":{"name":"Colorectal Disease","volume":"26 11","pages":"1883-1891"},"PeriodicalIF":2.9000,"publicationDate":"2024-09-18","publicationTypes":"Journal Article","fieldsOfStudy":null,"isOpenAccess":false,"openAccessPdf":"https://onlinelibrary.wiley.com/doi/epdf/10.1111/codi.17172","citationCount":"0","resultStr":"{\"title\":\"Splenic flexure adenocarcinoma: A national cohort analysis of extent of surgical resection and outcomes\",\"authors\":\"Julia F. Kohn, Sonja Boatman, Qi Wang, Schelomo Marmor, Imran Hassan, Robert D. Madoff, Wolfgang B. Gaertner, Paolo Goffredo\",\"doi\":\"10.1111/codi.17172\",\"DOIUrl\":null,\"url\":null,\"abstract\":\"<div>\\n \\n \\n <section>\\n \\n <h3> Aim</h3>\\n \\n <p>The optimal extent of resection for splenic flexure adenocarcinoma remains debated. These tumours straddle the left- and right-sided vasculature with lymphatic drainage in a watershed area; current guidelines recommend either segmental or extended colectomy. We analysed surgical management of splenic flexure tumours and compared outcomes between approaches.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Method</h3>\\n \\n <p>The Surveillance, Epidemiology and End Results database was searched for adults with Stage I–III splenic flexure adenocarcinoma, 2004–2019.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Results</h3>\\n \\n <p>Of 5238 patients, 55% underwent extended colectomy. Compared to segmental colectomy, these patients were more likely to have advanced stage. On multivariable analysis, age ≤ 65 years remained independently associated with extended colectomy. Although fewer nodes were examined in segmental colectomy (median 14 vs. 16, <i>p</i> < 0.001), the number of positive nodes (both, median 0 [interquartile ratio 0–2], <i>p</i> = 0.20) and the lymph node ratio were similar between cohorts. Surgical approach was not significantly associated with increased positive nodal yield in adjusted analyses. Five-year overall and disease-specific survival were 73% and 84% for segmental and 72% and 83% for extended colectomy (<i>p</i> > 0.4); these remained comparable after adjustment.</p>\\n </section>\\n \\n <section>\\n \\n <h3> Conclusions</h3>\\n \\n <p>Nationally, we observed similar rates of segmental and extended colectomy for splenic flexure adenocarcinoma. Extended colectomy was not more common in Stage III disease, indicating lack of stage migration, and was not associated with better oncological outcomes. These observations support current practice involving either approach, which should be tailored to patient-related factors and preferences, while considering technical aspects and quality of life.</p>\\n </section>\\n </div>\",\"PeriodicalId\":10512,\"journal\":{\"name\":\"Colorectal Disease\",\"volume\":\"26 11\",\"pages\":\"1883-1891\"},\"PeriodicalIF\":2.9000,\"publicationDate\":\"2024-09-18\",\"publicationTypes\":\"Journal Article\",\"fieldsOfStudy\":null,\"isOpenAccess\":false,\"openAccessPdf\":\"https://onlinelibrary.wiley.com/doi/epdf/10.1111/codi.17172\",\"citationCount\":\"0\",\"resultStr\":null,\"platform\":\"Semanticscholar\",\"paperid\":null,\"PeriodicalName\":\"Colorectal Disease\",\"FirstCategoryId\":\"3\",\"ListUrlMain\":\"https://onlinelibrary.wiley.com/doi/10.1111/codi.17172\",\"RegionNum\":3,\"RegionCategory\":\"医学\",\"ArticlePicture\":[],\"TitleCN\":null,\"AbstractTextCN\":null,\"PMCID\":null,\"EPubDate\":\"\",\"PubModel\":\"\",\"JCR\":\"Q2\",\"JCRName\":\"GASTROENTEROLOGY & HEPATOLOGY\",\"Score\":null,\"Total\":0}","platform":"Semanticscholar","paperid":null,"PeriodicalName":"Colorectal Disease","FirstCategoryId":"3","ListUrlMain":"https://onlinelibrary.wiley.com/doi/10.1111/codi.17172","RegionNum":3,"RegionCategory":"医学","ArticlePicture":[],"TitleCN":null,"AbstractTextCN":null,"PMCID":null,"EPubDate":"","PubModel":"","JCR":"Q2","JCRName":"GASTROENTEROLOGY & HEPATOLOGY","Score":null,"Total":0}
Splenic flexure adenocarcinoma: A national cohort analysis of extent of surgical resection and outcomes
Aim
The optimal extent of resection for splenic flexure adenocarcinoma remains debated. These tumours straddle the left- and right-sided vasculature with lymphatic drainage in a watershed area; current guidelines recommend either segmental or extended colectomy. We analysed surgical management of splenic flexure tumours and compared outcomes between approaches.
Method
The Surveillance, Epidemiology and End Results database was searched for adults with Stage I–III splenic flexure adenocarcinoma, 2004–2019.
Results
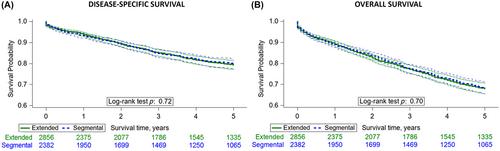
Of 5238 patients, 55% underwent extended colectomy. Compared to segmental colectomy, these patients were more likely to have advanced stage. On multivariable analysis, age ≤ 65 years remained independently associated with extended colectomy. Although fewer nodes were examined in segmental colectomy (median 14 vs. 16, p < 0.001), the number of positive nodes (both, median 0 [interquartile ratio 0–2], p = 0.20) and the lymph node ratio were similar between cohorts. Surgical approach was not significantly associated with increased positive nodal yield in adjusted analyses. Five-year overall and disease-specific survival were 73% and 84% for segmental and 72% and 83% for extended colectomy (p > 0.4); these remained comparable after adjustment.
Conclusions
Nationally, we observed similar rates of segmental and extended colectomy for splenic flexure adenocarcinoma. Extended colectomy was not more common in Stage III disease, indicating lack of stage migration, and was not associated with better oncological outcomes. These observations support current practice involving either approach, which should be tailored to patient-related factors and preferences, while considering technical aspects and quality of life.
期刊介绍:
Diseases of the colon and rectum are common and offer a number of exciting challenges. Clinical, diagnostic and basic science research is expanding rapidly. There is increasing demand from purchasers of health care and patients for clinicians to keep abreast of the latest research and developments, and to translate these into routine practice. Technological advances in diagnosis, surgical technique, new pharmaceuticals, molecular genetics and other basic sciences have transformed many aspects of how these diseases are managed. Such progress will accelerate.
Colorectal Disease offers a real benefit to subscribers and authors. It is first and foremost a vehicle for publishing original research relating to the demanding, rapidly expanding field of colorectal diseases.
Essential for surgeons, pathologists, oncologists, gastroenterologists and health professionals caring for patients with a disease of the lower GI tract, Colorectal Disease furthers education and inter-professional development by including regular review articles and discussions of current controversies.
Note that the journal does not usually accept paediatric surgical papers.

 求助内容:
求助内容: 应助结果提醒方式:
应助结果提醒方式:


